{kind=link}
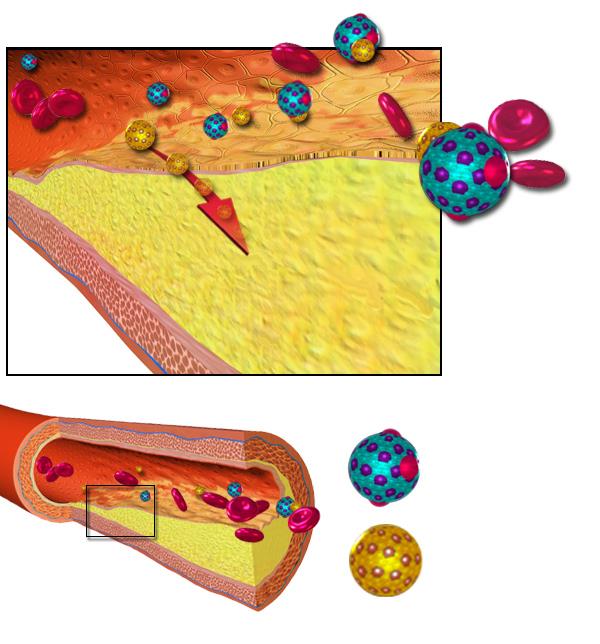
Pictured: The accepted theory of how cholesterol forms arterial plaques.
There is an organization that calls itself The International Network of Cholesterol Skeptics (THINCS). Its members “thinc” they are smarter than the average doctor. They “thinc” that cholesterol has nothing to do with cardiovascular disease and that we have been deluded into waging a “cholesterol campaign” for which the scientific evidence is non-existent. They say, “What we all oppose is that animal fat and high cholesterol play a role.” I find even the wording of this statement problematical: one does not usually hear scientists “opposing” matters of fact or non-fact. They go on to say, “The aim with this website is to inform our colleagues and the public that this idea is not supported by scientific evidence; in fact, for many years a huge number of scientific studies have directly contradicted it.”
They tell us about those contradicting studies; but they don’t tell us about the flaws in those studies, they misrepresent some of the results, and they don’t tell us about the many good studies that support the cholesterol/heart link. The issue is a complex one, and it is easy to find studies to support any claim. Good science is about weighing all the evidence pro and con before reaching a conclusion. As far as I can see, these folks have cherry-picked the literature to support an agenda. They seem to have a vendetta against statin drugs in particular.
The website solicits complaints of adverse effects from statin drugs. It features a petition to the WHO that you can sign requesting an investigation of statin side effects. It alleges that lowering cholesterol endangers the elderly. It provides “what the medical journals and newspapers won’t let you hear” – letters and papers that have been rejected for publication. It lists books, published papers and talks by its members. It solicits financial contributions to the cause.
This movement seems to have started with Uffe Ravnskov’s book The Cholesterol Myths, published in Swedish in 1991 and in English in 2000. That book has been severely criticized, for instance in The Skeptic’s Dictionary , where Bob Carroll points out some of the distortions and deceptive techniques found in the cholesterol skeptics’ arguments. A typical claim: “Cholesterol is highly protective against cancer, infection and atherosclerosis” and “high TC [total cholesterol] and LDL levels are beneficial at all ages.” These statements are not only false, they are potentially dangerous to the health of those who believe them.
I’ll admit there is a grain of truth in what they say. The public may falsely perceive cholesterol as some kind of “Great Satan” of heart disease, and diet has been overemphasized, and some doctors may be over-prescribing statins. But there is plenty of evidence from multiple avenues of research to show that high cholesterol is a risk factor for heart disease and that lowering it reduces risk. A Lancet article from December 2007 reviewed trials involving nearly a million people and found that “Total cholesterol was positively associated with IHD [ischemic heart disease] mortality in both middle and old age and at all blood pressure levels.”
Another Lancet meta-analysis of over 90.000 patients concluded “Statin therapy can safely reduce the 5-year incidence of major coronary events, coronary revascularisation, and stroke by about one fifth per mmol/L reduction in LDL cholesterol, largely irrespective of the initial lipid profile or other presenting characteristics. The absolute benefit relates chiefly to an individual’s absolute risk of such events and to the absolute reduction in LDL cholesterol achieved. These findings reinforce the need to consider prolonged statin treatment with substantial LDL cholesterol reductions in all patients at high risk of any type of major vascular event.”
Most doctors follow guidelines like those in a recent issue of American Family Physician. The article reviews the evidence, makes evidence-based practice recommendations for treating cholesterol abnormalities, and grades the quality of the evidence for each recommendation. It gives most of the recommendations the highest “A” rating.
Prevention is much more complex than just throwing statins at patients with high cholesterol. There are other ways to lower cholesterol, including weight loss. It makes a difference whether you are aiming for primary prevention (preventing disease in the first place) or secondary prevention (preventing further harm to someone who already has cardiovascular disease). A high LDL may not be as significant in a patient whose HDL (“good” cholesterol) is also high. Before prescribing, a good doctor looks at the whole patient: all the other risk factors, such as age, sex, weight, diet, exercise, family history, smoking, blood pressure, and past history. He looks at the risk/benefit ratio of statins in the patient’s particular situation. He considers the NNT (number needed to treat) to prevent one death or heart attack (which may vary from 5 to 333 depending on the situation). He looks at what other medications the patient is on, at the cost and convenience, at the patient’s personal philosophy and preferences. Ideally, the decision to use statins should be a joint decision of the patient and the doctor based on all the information available.
The cholesterol skeptics doubt that all-cause mortality can be reduced by statins. It clearly can for secondary prevention. In primary prevention, it at least reduces the rate of cardiovascular events. It’s not entirely clear whether the risk reduction with statins is due solely to the lowered cholesterol; statins may have other beneficial effects. But at least it appears that the degree of risk reduction can be measured by the degree of cholesterol lowering.
If you have the right genes, a high cholesterol level may not hurt you. And if you are at low risk, you can’t eat yourself into a heart attack just by overindulging in dietary fats and cholesterol. Some of the cholesterol skeptics’ objections are based on a misunderstanding of the relationship between dietary cholesterol and blood cholesterol levels. We used to recommend a low cholesterol diet, then a low fat diet, then a low saturated fat diet, and now we are concerned about trans-fats. We are refining our knowledge, and recommendations are changing accordingly. A reduced fat diet is still recommended for those with elevated blood cholesterol levels, but it may only lower the cholesterol level by 3 – 6%.
When I first went to the THINCS website, the first thing that popped up was a letter warning that statins caused cancer. When I checked the recent articles on “cancer” and “statins” in PubMed, most of the studies showed either no correlation with cancer or an apparent protective effect, especially for colorectal cancer and skin cancer. The NIH is studying statins for cancer prevention, and there is a plausible biologic rationale to support that concept (statins work against cellular functions that may help control tumor initiation, tumor growth and metastasis).
There are even suggestions that statins might benefit other diseases like Parkinson’s disease and Alzheimer’s.
The skeptics cite studies where elderly people with low cholesterol had worse outcomes, but the elderly often have confounding factors: in that age group low cholesterol can be a marker for inadequate diet and chronic disease. A 2008 study shows that “Statins reduce all-cause mortality in elderly patients and the magnitude of this effect is substantially larger than had been previously estimated.”
My impression is that the general trend of recent statin studies in the better journals has been to show even more efficacy and fewer side effects than previously thought. For instance, the 2007 West of Scotland Coronary Prevention Study, reported in the New England Journal of Medicine was very encouraging.
The cholesterol skeptics’ website rejects the consensus of medical science, saying that consensus is politics, not science. I beg to differ. Consensus based on opinion is politics. Consensus based on the evidence is an integral part of the scientific enterprise: when the evidence is convincing, the majority will be convinced.
Dissent, debate, and questioning the status quo are important in keeping science honest, but science doesn’t advance through activist groups like this. We didn’t need an “X-Ray Skeptics” group to realize that routine annual chest x-rays were a bad idea; we saw the evidence and stopped x-raying everybody.
We are still struggling to understand all the ins and outs of preventing cardiovascular disease. Current guidelines have been criticized because they are often based on extrapolations and on insufficient data about actual outcome. A letter to the editor of the American Family Physician compared guidelines in six different countries, and found that the American guidelines would save a few more lives but only at much greater expense: 198 patients treated at an expense of over $198,000 to prevent one death. I’m sure we’ve gotten some things wrong, and our present approach will surely be revised as we continue to learn. But to reject the cholesterol connection and statins entirely is to throw the baby out with the bathwater. In my opinion, THINCS is spreading misinformation that could lead patients to refuse treatment that might prolong their life or at least prevent heart attacks and strokes.