
{kind=link}
As I like to bore my readers by endlessly repeating it, there’s nothing new under the sun when it comes to antivaccine misinformation. Every single antivax trope about COVID-19 vaccines that so surprised many of my colleagues when it first showed up has been directly traceable to old antivax tropes going back decades. That includes claims that vaccines somehow “permanently alter your DNA”—”homologous recombinaltion tiniker” and “molecular mimicry,” anyone?—and thereby cause a host of problems, such as autoimmune diseases and even cancer. Last week, I discussed how antivaxxers twisted a study to falsely blame COVID-19 vaccines for “accelerated aging” leading to—you guessed it!—cancer. This week, I’m going to look at some more of the “evidence” being promoted by antivaxxers as “proof” that the evil COVID-19 vaccines are killing younger people left and right by causing cancer, a 14,000% increase in “turbo cancer,” even.
Before I dig in, though, let me just remind everyone that just because in the realm of antivax disinformation “everything old is new again” with COVID-19 doesn’t mean that the COVID-19 vaccine-related versions of old antivax tropes haven’t gained new twists. In the case of the antivax claim that vaccines cause cancer, the new COVID vaccine-related twist is that the new mRNA-based COVID-19 vaccines don’t just cause something as mundane as your run-of-the-mill cancers of the sort that, taken together, are the second leading cause of death after cardiovascular disease. Oh, no. They’re too awful to cause just run-of-the-mill average cancers. They’re such super-powerful magical carcinogens that they cause “turbo cancers” described by antivaxxers as cancers that develop and grow so rapidly as to be essentially untreatable or cancers, previously in remission, that spring back to life, thanks to the mRNA itself or minute quantities of contaminant plasmid DNA fragments from the plasmid used to generate the mRNA left over from the manufacturing process. Never mind that we know from the atomic bombings at Hiroshima and Nagasaki that the shortest period for the development of cancer after exposure to one of the most potent carcinogens known (ionizing radiation) is around two years for leukemias and ten years for solid cancers. In comparison, COVID-19 vaccines have only been around a little more than three years and the claims of “turbo cancers” started less than two years after they were first granted emergency use authorization (EUA). Tellingly, for the most part, it is not “turbo leukemias” being blamed on the vaccines, but “turbo” solid cancers of the type that take over 10 years to develop.
Of course, this latest “evidence dump” billed as “TURBO CANCER Literature is growing rapidly – 6 new COVID-19 Vaccine Turbo Cancer papers published in April 2024 – 26 total – the dam is breaking and it will take Pfizer & Moderna with it“) comes from disgraced and delicensed nuclear medicine doc Dr. William Makis, one of the originators and now one of the foremost promoters of the “turbo cancer” lie. I’m not going to cover all of the articles, although I note that I’ve already discussed some of them and why they are not good evidence for a link between COVID-19 vaccines and cancer, “turbo cancer” or otherwise. Part of the reason Makis’ post got my attention is because one of the studies is a preprint published by someone whom I’ve discussed before, a director of a cancer center who has demonstrated himself to be far too receptive to fancifully implausible claims of a “biological mechanism” to explain how COVID-19 vaccines can supposedly integrate into genomic DNA and thereby cause cancer, even though he should really, really know better. (Worse, he doubled down in response to even polite, respectful criticism.) I’m referring to Dr. Wafik El-Deiry, someone whom I actually quite admired back in the 1990s as a graduate student and later postdoc, indeed, from then until relatively recently, when I noticed him granting an interview to an antivax propagandist. Let’s just say that I’ll agree that the “turbo cancer” literature is growing, rather like maggots on a rotting wound of bad science.
Et tu, Dr. El-Deiry?
That Dr. William Makis is an antivax quack is a point that I’ve made multiple times here and at my not-so-super-secret other blog, bringing the receipts, of course, that led me to that unfortunate conclusion. As for Prof. Wafik El-Deiry, I’ve noted before how he is an unexpected source to have been so credulous about claims of someone like Phillip Buckhauts, who has been furiously promoting claims that fragments of the SV40 promoter in the fragments of plasmid DNA left over from the vaccine manufacturing process are “integrating” with genomic DNA and causing cancer. That’s because Dr. El-Deiry is an oncologist and cancer biologist whose work influenced me as a graduate student 20 years ago and who is now the director of the Legorreta Cancer Center at Brown University. He’s been a big name in p53 research for 30 years. I hadn’t heard much from him for several months, but now apparently he’s trying to publish an article describing experiments that, well, look at the title of his preprint: SARS-CoV-2 spike S2 subunit inhibits p53 activation of p21(WAF1), TRAIL Death Receptor DR5 and MDM2 proteins in cancer cells, posted a week ago to the bioRxiv preprint server.
In fairness, one could argue that this study isn’t about the vaccine at all, but rather SARS-CoV-2 infection, and that this is just another example of an antivaxxer like Dr. Makis willfully misinterpreting a study to link it to the “turbo cancer” narrative, an example of which I just discussed last week. Maybe, although antivaxxers seem to interpret the paper otherwise, given the answers to his Tweet about the preprint:
Again, this could just be antivaxxers willfully misinterpreting, but…
Before I get into the experiments, let’s just unpack some of the abstract:
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and COVID-19 infection has led to worsened outcomes for patients with cancer.
This is, of course, true enough, but, I suspect, not for the reasons that Dr. El-Deiry is going to argue. Rather, any severe infectious disease is going to lead to poorer outcomes for patients with cancer, if only because of the disruption of treatment and by making them sick from a cause other than the cancer. Still, do go on, Dr. El-Deiry:
SARS-CoV-2 spike protein mediates host cell infection and cell-cell fusion that causes stabilization of tumor suppressor p53 protein
Given that p53 is a tumor suppressor, the “guardian of the genome,” even, one might think that this would actually make one less susceptible to cancer; that is, if it really happens. That’s why I had to go to the actual text to see what Dr. El-Deiry meant:
An in-silico analysis using HADDOCK 2.2 software previously suggested that p53 and BRCA1/2 may interact with the heptic repeat-2 region of the S2 subunit through C-terminal domain [6]. DNA damage or therapy-induced tumor suppressor p53 protein transcriptionally activates genes leading to multiple effects preserving genome integrity, altering metabolism, immune response, cell cycle, DNA repair, cell growth and cell apoptosis to prevent or eliminate transformed cells [7]. Loss of p53 function increases the incidence of carcinogen-induced tumorigenesis and drives chemo-resistance [8]. SARS-CoV-2 infection has been found to alter p53 stabilization. The previous studies have shown that SARS-CoV-2 spike in particular plays a role to stabilize and activate p53 by mediating cell-cell fusion or induction of ROS in host cells during SARS-CoV-2 virus infection [9, 10]. In response to cellular stress, activated p53 regulates specific gene expression, including MDM2 (E3 ligase). MDM2, in turn, binds to p53 and triggers p53 ubiquitination and proteasomal degradation [11], while interruption of MDM2-p53 interaction leads to p53 stabilization. Thus, a putative interaction between SARS-CoV-2 spike, p53 and p53 related signaling pathways following SARS-CoV-2 infection could impact cellular homeostasis, tumorigenic pathways, and/or response to cancer therapeutics.
I note that the study dates back to 2020 and that I’ve previously noted that the findings of this study, even if the study pans out, said nothing about the vaccine; rather, it was about persistent SARS-CoV-2 infection, not vaccination. The vaccine only transiently produces the spike protein, which is rapidly externalized. If it weren’t externalized, then it wouldn’t be able to provoke an immune response. p53 is not just an intracellular protein, but, unlike the spike protein, is primarily a protein of the nucleus. Vaccination is transient by nature, and, even if this proposed interaction were relevant, would require prolonged interaction between spike and p53. In fairness, at this point, Dr. El-Deiry hasn’t mentioned the vaccine…yet. He’s only mentioned SARS-CoV-2 infection. Moreover, what he seems to be saying is that the spike protein activates p53, not deactivates it, the latter of which being necessary for cancer formation. In fact, almost nowhere does Dr. El-Deiry even mention the vaccine. However, where he does mention it, I think he gives the game away, as you will see.
I will also note that this preprint is a bit thin in that it only has four figures. That doesn’t mean that it’s wrong or even not good science, just that not a lot of information is there. Personally, I actually wish more journals would publish shorter, punchier papers with only one or two key findings, rather than insisting on ten-figure, many thousand word epics. Be that as it may, let’s summarize the key findings. First, however, note that we can’t describe the findings without examining the methods first, starting with the cell lines used: human lung cancer cells H460, breast cancer cells MCF7, colorectal cancer cells HCT116 (p53 wild-type or p53-null), and sarcoma cells U2OS with p53-knockout (U2OS-P53KO). One can see why he would choose some of these cell lines, particularly the ones lacking p53, if one wants to test whether SARS-CoV-2 spike protein interacts with p53. In any event, these cells were transfected with a plasmid designed to produce the S2 unit of the spike protein:
The plasmids pcDNA3.1-SARS2-spike (#145032) and p-CMV-Neo-Bam-p53wt (#16434) were obtained from Addgene.
Before I even look at the results of the experiments in which this plasmid is used, I had questions. Maybe some of my more advanced molecular biology colleagues more familiar with SARS-CoV-2 than I can help out. Even a surgeon-molecular biologist like myself knows that the SARs-CoV-2 spike protein is made of two subunits, S1 and S2. The S1 subunit contains a receptor-binding domain that recognizes and binds to the host receptor angiotensin-converting enzyme 2 (ACE2), while the S2 subunit mediates viral cell membrane fusion. Moreover, the inactive S protein exists as a single peptide, but is activated by cleavage into S1 and S2 by cellular proteases during infection.
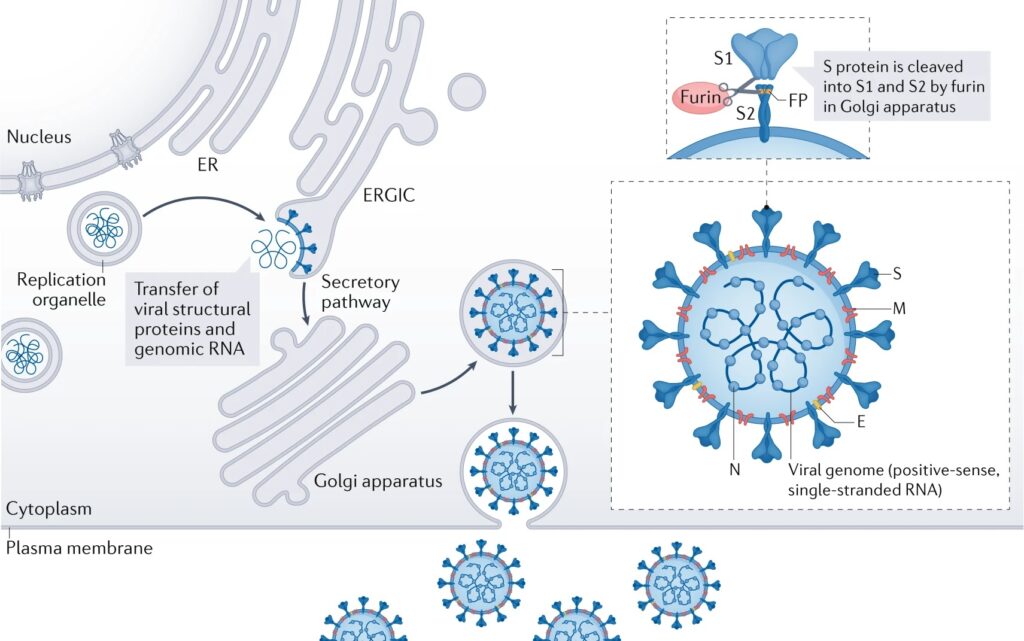
If you look at the construct on the company’s website, it states that it encodes the full length spike protein, which makes me wonder: When the protein is made in cancer cells, is it processed and cleaved into its subunits S1 and S2 at its furin cleavage site the way that a normal spike protein is? The reason I ask this is because at some points in the manuscript the product made by the plasmid is described as S2, while in other parts it’s described as spike. We know that the spike protein is 1,273 amino acids in length. A virologist whom I asked about this mentioned that throughout the paper there are references to “S2 expression,” wondering whether this was just sloppy terminology or whether another reagent was used. He also wondered whether cancer cells—remember, all the cell lines used are cancer cells—can proteolytically process the S protein into S1 and S2? I don’t know the answer to that question, but if I were reviewing the paper I would require that the authors answer the question, either with the literature or with additional control experiments.
Let’s just describe what the study shows as described by its authors. The authors did an immunoprecipitation experiment, which involves using antibodies to precipitate a protein, but used a somewhat more complex version that can determine if other proteins are attached to the precipitated protein. For simple IP, in brief, an antibody (monoclonal or polyclonal) against a specific target protein is used to form an immune complex with that target in a sample, such as a cell lysate. The immune complex is then captured, or precipitated, on a beaded support to which an antibody-binding protein is immobilized (such as Protein A or G). Any proteins not precipitated on the beads are then washed away. Finally, the protein is separated from the antibody and run through a polyacrylamide gel for Western blot detection.
In brief, First, here’s a diagram describing the basic concept of immunoprecipitation (IP):

But what about co-precipitation? The main difference is that what is precipitated and analyzed are complexes of the two different proteins:

You don’t need to know the fine details, but rather to understand the co-IP is a test to see if two proteins bind to each other and, if so, by how much. As I learned myself during graduate school and later during my fellowship research, IP can be a tricky technique, co-IP even more so. It can be influenced by a lot of things and the co-precipitation of two proteins doesn’t necessarily in and of itself demonstrate that two proteins physically interact with each other. For example, they could just be in the same subcellular fraction.
The immunoprecipitation experiments reported appear to show that there was reduced interaction between p53 and a protein called MDM2 following SARS-CoV-2 spike S2 overexpression in these cell lines. More specifically, the IP assay showed that MDM2 protein bound to p53 in the cells, while cells with “SARS-CoV-2 spike S2 subunit” overexpression displayed reduced amounts of MDM2 bound to p53 when compared to what was observed with the empty vector transfection control. In some experiments, cancer cells were exposed to cis-platinum compounds, which induce double-stranded DNA breaks and activate the DNA repair system in cells, as evidenced by increased activated p53. Since MDMs and p53 are known to interact with each other, the question of whether MDM2 actually binds to p53 itself is not so much an issue. However, what is interesting is that the paper itself shows that p53 and the S2 protein localize in different parts of the cell, and p53 does not co-preciptate with SARS-CoV-2 spike S2:
Our observations from lack of co-immunoprecipitation between p53 and the SARS-CoV-2 spike S2 protein subunit are consistent with different cellular locations of SARS-CoV-2 spike S2 and p53 in the cancer cells treated with cisplatin (Figure 1C). The immunofluorescence imaging showed that the majority of p53 was localized in the nuclei, while the majority of SARS-CoV-2 spike S2 subunit was localized in the cytoplasm in H460 cells treated with cisplatin (Figure 1C). These results do not demonstrate SARS-CoV-2-spike S2 subunit protein binding to wild-type p53 in cancer cells either in the absence or presence of cisplatin treatment. As this is a protein subunit, and some small amount of nuclear staining is observed, we cannot exclude that spike S2 can gain access to the nucleus or that intact spike could do so as well.
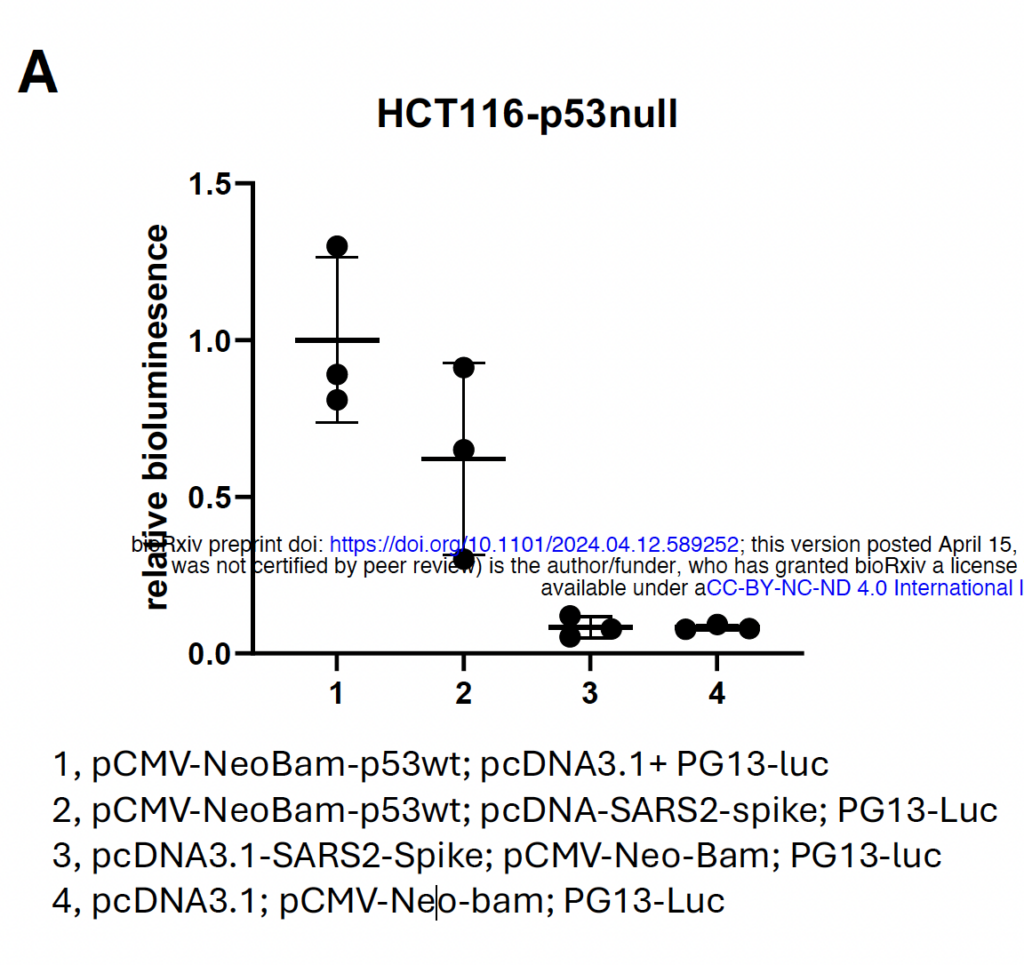
In additional experiments, it was shown that transfection of cells that do not express any p53 with the plasmid expressing p53 ± pcDNA3.1-SARS2-spike (the plasmid making spike) resulted in decreased transcriptional activity by p53, specifically as measured by co-transfection with a PG13-luciferase reporter gene. This particular plasmid contains 13 copies of the p53 binding site attached to the gene for luciferase. Basically, the more active p53 in a cell, the more bioluminescence will be measured. Now, I know from personal experience that these experiments are also tricky to do, but I will admit that this figure is fairly convincing that, however it does it, the presence of S2/spike does appear to decrease the activity of p53 in the cell:
But what does this have to do with cancer? Well, Dr. El-Deiry takes it back to p21, one of the genes turned on by p53 whose function is to induce cell cycle arrest, and finds that p21 doesn’t increase nearly as much in response to cis-platinum chemotherapy in cells transfected with pcDNA3.1-SARS2-spike as it does in cells transfected with control empty vector even though p53 levels increase by the same amount. Similar results were shown with TRAIL Death Receptor DR5 (which contributes to apoptosis or programmed cell death), and MDM2.
So what does it all mean? Hell if I know. First of all, these studies were all done in cancer cells, not normal cells. The authors note that their results differ from other reports:
Our findings differ from previous reports that have shown that SARS-CoV-2 spike stabilized p53 and activated p53 [9, 10]. In the previous studies, the p53 activation and stabilization was caused by the spike-ACE2 mediated cell-cell fusion and an increase in ROS in cancer or normal cells [9, 10].
One of the studies cited was done in retinal pigment epithelial (RPE) cells, which are not cancer cells, which could make a difference, while the other study included human tissue from postmortem examinations, but did include cancer cell lines and non-cancer cell lines. In any event, there are also a number of weaknesses in this study as well, which, in fairness, the authors acknowledge. One is a biggie:
We have not conducted in vivo experiments and some of our experiments lack additional controls such as in flow analysis or by looking at kinetics of cell cycle checkpoint regulation. We have not evaluated normal cells such as airway, muscle, immune, brain or intestinal cells. Cycling vs quiescent cells are also important to investigate for potential differential effects of spike or other SARS-CoV-2 proteins. We have not investigated immune cell interactions such as NK or T-cells in our experiments where spike S2 protein was overexpressed in culture. These would all be reasonable early future directions.
“Some of our experiments lack additional controls”? Perhaps those controls should have been done for this manuscript. Perhaps the authors should have looked at cycling versus quiescent (non growing) cells. Maybe the authors should have looked at some normal cells, such as airway, muscle, immune, brain, or intestinal cells. Perhaps in vivo mouse experiments should have been done. Maybe some of these experiments are being done for the submitted version and, for some reason, Dr. El-Deiry was anxious for as many people as possible to see this.
So far, a case can be made that this is just another paper being intentionally misinterpreted by antivaxxers as evidence for “turbo cancer.” In reality all this paper shows is that, in cell culture, it’s possible that SARS-CoV-2 infection might interfere with p53 activity. Of course, in cancers in which p53 is already inactivated or mutated, these findings would likely have little applicability. After all, p53 is already mutated and nonfunctional in these cancers. Would these findings tell us anything about how SARS-CoV-2 might affect cancer response to chemotherapy? Maybe to cis-platinum in certain cell types, but that’s about it so far. Basically, overall it’s a study in cancer cells in dishes using an artificial system in which plasmids coding the relevant proteins using a liposome-based system to introduce the DNA into the cells, after which the cells were broken open and the extracts subjected to immunoprecipitation.
Taking the most charitable view of the study, I find it mildly interesting, but far too preliminary to make much of a conclusion about and missing relevant controls, which is probably one reason why it’s a preprint rather than submitted to the high quality journals in which Dr. El-Deiry has usually published over the last 30 years. I’m not sure that it adds much to what we already know about spike protein and SARS-CoV-2 infection.
However:
Our results have implications for the biological effects of spike S2 subunit in human cells whether spike is present due to primary COVID-19 infection or due to mRNA vaccines where its expression is used to promote anti-viral immunity. A perturbed p53 pathway is concerning but also complicated in sorting out since cellular transformation and cancer are a multi-step process that evolves over time. Further detailed studies can more fully characterize the effects of spike, as well as structural determinants within the protein for interaction between the DNA damage sensing and response pathways as well as the p53 tumor suppressing pathway. With respect to the p53 pathway, further studies are needed to unravel how less MDM2 is bound to p53 in the presence of spike and the mechanisms underlying reduced p21(WAF10), TRAIL Death Receptor DR5 as well as MDM2 under conditions where there is less degradation of p53 due to reduced interaction with MDM2.
“Whether spike is present due to primary COVID-19 infection or due to mRNA vaccines where its expression is used to promote anti-viral immunity”? Antivaxxers have noticed:
Meanwhile:
The rest of the Tweet:
But clearly loss of p53 is associated with cancer over time. It is a difficult area when one discusses “causes.” It’s like cause of death. There’s an immediate cause but there can be many contributing factors.
We need more science and research to have a solid knowledge base and concrete plans to address risks. Research takes time, costs money, and needs to be better supported in the US to continue to have increasing impact on health, quality of life and even costs of healthcare.
So did Dr. El-Deiry mean his mention of the vaccine, which was almost a throwaway, as a dog whistle to the antivax movement blaming the COVID-19 for “turbo cancer”? Who knows? Only he can answer that for sure. I do know that, given his past history of credulity to the idea that minute amounts of contaminating DNA from the COVID-19 vaccine, SV40 in particular, cause cancer, antivaxxers were guaranteed to latch onto this paper as more evidence for “turbo cancer,” whether Dr. El-Deiry meant it that way or not.
But what about the other “evidence”?
I spent longer than I had anticipated discussing Dr. El-Deiry’s paper, mainly because it’s actual basic bench science and I don’t get to discuss basic bench science as much as I like. One other paper that I definitely haven’t discussed before was cited by Dr. Makis that I might well have to discuss, although the discussion might be done at my not-so-super secret other blog. As for the other “evidence,” it largely consists of case reports, such as this preprint (leukemia in a young woman after the second dose of the Moderna vaccine, as though young people never got leukemia before the vaccine) this paper (hemophagocytic lymphohistiocytosis with intravascular large B-cell lymphoma after her second dose in the presence of immunosuppression due to lupus), and this case report (Primary Cutaneous Adenoid Cystic Carcinoma in a Rare Location With an Immune Response to a BNT162b2 Vaccine), none of which actually show that the vaccine caused the cancer.
Again, I am not saying that every scientifically reasonable concern about vaccines that have been distributed to billions of people now should not be the subject of scientific investigation. What I differ about is what constitutes a scientifically reasonable concern. Dr. Makis’ “concerns” are anything but reasonable, while I’ve found Dr. El-Deiry to be either willfully or just painfully naive. Either way, he still seems utterly unaware of the well-funded networks that exist to spread misinformation and/or he is sympathetic to the misinformation being spread. Worse, his latest study doesn’t really provide any new information of value with respect to the question of whether SARS-CoV-2 infection has any effect on cancer risk or development.
ADDENDUM: I must admit that, after I finished this post, I wondered whether I was too hard on Dr. El-Deiry, but then he tagged me with this on Facebook:
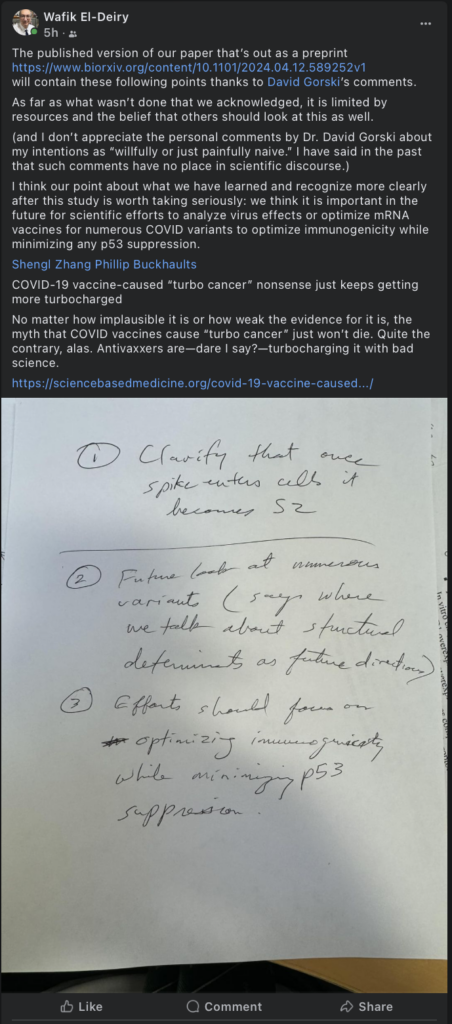
Also, let me just mention that this isn’t just about science, and I stand by my assessment of Dr. El-Deiry, although I’m starting to have a different doubt. Now I’m wondering if, based on my memories of reading and admiring his studies in the 1990s and 2000s, I’m making too great an effort to bend over backwards to be respectful. I mean, tagging Phillip Buckhaults, who has promoted based on bad science fear mongering about SV40 sequences from residual plasmid DNA in the vaccines? Seriously?