{kind=link}
I wonder how many people have heard that chiropractic neck adjustments can cause strokes. It isn’t exactly common knowledge. One organization is trying to raise public awareness through signs on the side of city buses (Injured by a Chiropractor? Call this number) and through TV commercials. I had never heard about this phenomenon myself until a few years ago, when I heard it mentioned on an episode of Alan Alda’s Scientific American Frontiers. I questioned his accuracy, but I quickly found confirmation in the medical literature.
A typical case was that of 24 year old Kristi Bedenbaugh who saw her chiropractor for sinus headaches. During a neck manipulation she suffered a brain stem stroke and she died three days later. Autopsy revealed that the manipulation had split the inside walls of both of her vertebral arteries, causing the walls to balloon and block the blood supply to the lower part of her brain. Additional studies concluded that blood clots had formed on the days the manipulation took place. The chiropractor later paid a $1000 fine.
The two vertebral arteries run straight up the back of the neck passing through holes in the sides of each neck vertebra. When the head
turns, the “tethered” artery is drastically kinked: 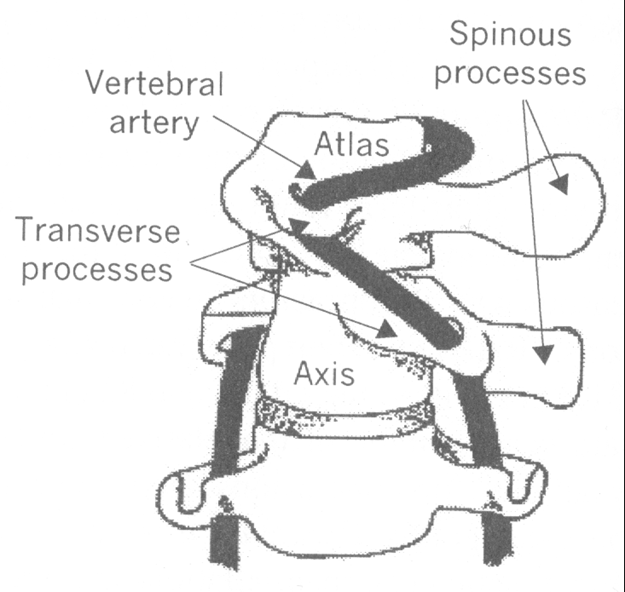
Because of this kinking, it is particularly susceptible to injury. Even a simple thing like extending the neck back over the basin for hair washing at the beauty salon has been known to cause a stroke. The artery is elastic, but with hardening of the arteries, with cholesterol plaques, with trauma (like automobile accidents) or simply with rapid stretching, the delicate lining of the artery can tear. It is easy to imagine how a rapid, forceful thrust by a chiropractor could cause damage.
Sometimes the damage is immediate and the patient collapses on the chiropractor’s table. Sometimes mild symptoms start immediately and progress after the patient leaves the chiropractor’s office. Sometimes the tear is a small one and it clots over; then days later the clot breaks loose, travels to the brain and causes a delayed stroke. By this time, the patient may not connect his sudden collapse to the previous visit to the chiropractor.
Chiropractors are well aware of the risk. They discuss it in their journals and online forums. They have tried to find ways to screen patients for high risk, but there is no reliable way to do so. Strokes are a major reason for chiropractic malpractice insurance payouts – 9% of claims paid by the major chiropractic insurer in 2002, the only year for which I was able to find statistics. Some chiropractors are now asking patients to sign an informed consent form before manipulations. If asked, most chiropractors downplay the risk, saying it occurs in less than one in a million manipulations. Many (perhaps most) chiropractors do not mention the risk at all.
Most alarming: some chiropractors perform these neck adjustments with no warning and without permission. I met a woman who still walks with a limp and has other residual impairments from a chiropractic stroke. She went to her chiropractor for a shoulder problem and thought he was going to massage her shoulder muscles. She did not want him to manipulate her neck, did not give him permission, and didn’t realize what he was doing until he suddenly twisted her neck. She collapsed on the table and nearly died.
How often can a stroke be attributed to neck manipulation? We really don’t know. Estimates have varied from one in ten million manipulations to one in 40,000. I should clarify that only one specific type of stroke, basilar stroke, has been linked to chiropractic. It has been estimated that about 20% of all basilar strokes are due to spinal manipulations. This would work out to about 1300 a year in the U.S. But we just don’t know, because it has not been properly studied. Carotid artery strokes have also been reported after chiropractic treatments. Chiropractors do not follow up on every patient. Patients who have delayed strokes may never see their chiropractor again, so chiropractors would naturally tend to underestimate the risk. Many of these diagnoses are missed because the vertebral arteries are not typically examined on autopsy.
One study of patients under the age of 45 who had this kind of stroke showed that they were 5 times more likely to have visited a chiropractor in the preceding week than control patients. In the past, neurologists treating stroke patients simply did not ask patients about chiropractic; and when they started asking, they started finding. There have been deaths. There have been court cases. In 2002, a group of Canadian neurologists issued a statement of concern to the public, recommending vigilance, education, informed consent, and other measures to protect the public. Awareness is rising, and injured patients have formed organizations in the US, Canada, and the UK both for support and for litigation.
Defensive chiropractors have tried to counteract the growing body of evidence with studies like this one, which concluded that “SMT [Spinal Manipulation Therapy] resulted in strains to the VA [Vertebral Artery] that were almost an order of magnitude lower than the strains required to mechanically disrupt it. We conclude that under normal circumstances, a single typical (high-velocity/low amplitude) SMT thrust is very unlikely to mechanically disrupt the VA.” That’s certainly true. It is unlikely. Under normal circumstances. But it does happen.
They tell us that the stroke would have happened anyway. Maybe. We don’t have any way of knowing. But when the patient collapses immediately after the neck is twisted, I think we can say the stroke wouldn’t have happened at that time without the manipulation. Given a choice of sooner or later, later is good.
They tell us that other treatments for neck pain, like NSAIDs, also carry dangers. Patients have developed bleeding ulcers and died from taking aspirin. That’s very true, but they are invoking the logical fallacy known as tu quoque: just because something else is dangerous too, that doesn’t make neck manipulation any less dangerous. And comparing the dangers of two treatments doesn’t mean there aren’t other options that are safer than either of them.
Until really good studies are done, we simply don’t know the magnitude of the risk; but we are reasonably confident there is a risk. Now, let’s measure that risk against the benefits. Some chiropractors are doing neck adjustments on 90% of their patients for everything from ear infections to low back pain. There are lots of testimonials, but no POEMS (patient-oriented evidence that matters) and no evidence of any long-term benefit or any advantage over other treatments. The only thing neck manipulations have been shown to help with is mechanical neck pain, and a recent Cochrane review did not find that manipulation was any better than simple mobilization treatments. If there is no benefit, isn’t any degree of risk too much?
There are plenty of other options for treating mechanical neck pain for those who prefer not to take pain pills. The cervical spine can be gently mobilized with physical therapy methods that have not been linked to stroke. Heat, massage, tincture of time, exercises and other measures may offer symptomatic relief with no associated risks.
“Don’t ever let a chiropractor touch your neck “is the safest advice; but we can’t expect everyone to accept it. Some patients have had good experiences with neck manipulations and will continue to ask for them. We can’t presume to dictate to others. If someone judges that there is a one in a million risk of a stroke and is willing to take that risk, he has every right to do so. I think people have the right to engage in risky behaviors like skydiving and smoking cigarettes. I just think they deserve to know there is a risk, and to have some idea how much of a risk it is. I suspect the general public doesn’t know the facts about neck manipulation.
I wonder if Laurie Jean Mathiason knew neck manipulations could cause strokes. This 20 year old girl had a tailbone injury and sought out a chiropractor who manipulated her neck. Yes, her neck – to fix her tailbone! She fell into a coma and died three days later. Her visit to the chiropractor might qualify her for a Darwin Award. In my opinion, it qualifies as a tragedy and a crime.
For more information and links see: http://www.quackwatch.org/01QuackeryRelatedTopics/chirostroke.html