{kind=link}

Four weeks ago, I wrote a post in which I explained why wearing a bra does not cause breast cancer. After I had finished the post, it occurred to me that I should have saved that post for now, given that October is Breast Cancer Awareness Month. The reason is that, like clockwork, pretty much every year around this time articles touting various myths about breast cancer will go viral, circulating on social media like Facebook, Twitter, Pinterest, and Tumblr like so many giant spider-microbes on the moon on Saturday. Sometimes, they’re new articles. Sometimes they’re old articles that, like the killer at the end of a slasher film, seem to have died but always come back for another attack, if not immediately, then when the next movie comes out.
So I thought that this October I should take at least a couple of them on, although I can’t guarantee that I’ll stick to the topic of breast cancer myths for the whole month. After all, our “atavistic oncology” crank (you remember him, don’t you?) is agitating in the comments and e-mailing his latest “challenge” to my dean, other universities, and me. It was almost enough for me to put this post on hold for a week and respond to our insistent little friend’s latest “evidence,” but for now I’ll just tell Dr. Frank Arguello, “Be very careful what you ask for. You might just get it.” Maybe next week. Or maybe on my not-so-super-secret other blog. Or maybe never. Because Dr. Arguello has officially begun to bore me.
In the meantime, I’m going to stick with the original plan, at least for now.
So, first up this week is a myth that I can’t believe that I haven’t covered in depth sometime during the nearly seven years of this blog’s existence, other than in passing a couple of times, even though it’s a topic that deserves its own post. I’m referring to the claim that antiperspirants cause breast cancer. I bet you’ve seen articles like this oldie but not so goodie from über-quack Joe Mercola entitled “Are Aluminum-Containing Antiperspirants Contributing To Breast Cancer In Women?” or this older and even moldier article from seven years ago entitled “Why women should avoid using anti-perspirants that could cause breast cancer” or this one from last year entitled “Attention Deodorant Users: New Studies Link Aluminum To Breast Cancer“. Surprisingly, I haven’t found that many from this year yet. (Maybe the Ebola scare is distracting the usual suspects and diverting their efforts.) The same ones, however, keep reappearing every year, and they’re all based on the same sorts of claims and the same studies. So let’s dig in, shall we?
Spaced…1999
It all began, at least as far as it is possible to figure out the precise origin of any recurring myth about health, with an e-mail dating back to 1999, as described on Snopes.com:
BREAST CANCER PREVENTION
Not just for women — men don’t forget to tell mom, cousins, etc. Deodorants (non-antiperspirants) are very hard to find but there are a few out there.
I just got information from a health seminar that I would like to share.
The leading cause of breast cancer is the use of anti-perspirant.
What? Yes ANTI-PERSPIRANT. Most of the products out there are an anti-perspirant/deodorant combination so go home and check your labels.
Deodorant is fine, anti-perspirant is not. Here’s why:
The human body has a few areas that it uses to purge toxins; behind the knees, behind the ears, groin area, and armpits. The toxins are purged in the form of perspiration.
Anti-perspirant, as the name clearly indicates, prevents you from perspiring, thereby inhibiting the body from purging toxins from below the armpits. These toxins do not just magically disappear. Instead, the body deposits them in the lymph nodes below the arms since it cannot sweat them out. This causes a high concentration of toxins and leads to cell mutations: a.k.a. CANCER. Nearly all breast cancer tumors occur in the upper outside quadrant of the breast area. This is precisely where the lymph nodes are located.
Additionally, men are less likely (but not completely exempt) to develop breast cancer prompted by anti-perspirant usage because most of the anti-perspirant product is caught in their hair and is not directly applied to the skin. Women who apply anti-perspirant right after shaving increase the risk further because shaving causes almost imperceptible nicks in the skin which give the chemicals entrance into the body from the armpit area.
PLEASE pass this along to anyone you care about. Breast Cancer is becoming frighteningly common. This awareness may save lives. If you are skeptical about these findings, I urge you to do some research for yourself. You will arrive at the same conclusions, I assure you.
The origin of this myth is rooted in a typical misunderstanding of biology that regular readers probably recognized immediately, namely the issue of “toxins.” It is simply not true that apocrine sweat glands (the variety of sweat gland that are found predominately under the arm and in the groin area that can produce substances that the bacteria on the skin feast upon to make the characteristic stinky aroma) are a major source of “detoxification,” nor is there any compelling evidence that blocking these sweat glands, which is how aluminum-containing antiperspirants tend to work, results in the accumulation of “toxins” under the arm. There’s also another misunderstanding here. If, as is described, nicks from shaving the armpit allow the evil chemicals from the antiperspirant to get in, what would be far more likely to happen than what this e-mail assumes is either that (1) the chemicals would get into the bloodstream and disperse throughout the body, highly diluted, or (2) the chemicals would remain in the dermis (the layer of the skin immediately below the epidermis, which is usually all that is nicked by shaving). In the case of #2, let’s just put it this way: If the skin was cut all the way through the dermis that would be one hell of a cut. Also, with the use of modern safety razors, a cut that goes more than just a little bit into the dermis is highly unlikely. So, if #2 were true, we’d expect an elevated risk of skin cancer in the area, not breast cancer, because there is no plausible mechanism by which the evil chemicals from the antiperspirant to get much beyond the dermis, much less to accumulate in the breast tissue. Given that the apocrine sweat glands are located in the subcutis or at most the superficial subcutaneous fat, the same would be true even if antiperspirants caused toxins that would otherwise escape through sweat to be bottled up in the sweat gland.
So, right off the bat, we see a plausibility problem to this hypothesis. Of course, we’re not talking homeopathy-level implausibility here, but it’s hard to imagine a logical, science-based mechanism whereby antiperspirants could lead to a highly elevated risk of breast cancer in just one quadrant, the upper outer quadrant, of the breast.
But what about the claim that “nearly all” cancers occur in the upper outer quadrant of the breast and the observation that that is “precisely where the lymph nodes are located.” Well, yes and no. First off, this observation seems to be confusing sweat glands and lymph nodes, as though blocking off sweat glands would cause backups of those mysterious, never identified “toxins” in the lymph nodes. They’re two different things, and lymph nodes are not connected to the sweat glands, as this e-mail (and many articles claiming that antiperspirants cause breast cancer) seems to assume.
Also, it is not true that “nearly all” breast cancers are in the upper outer quadrant (the quadrant closest to the armpit), although it is true that there is a propensity for breast cancer to appear there first. Why is this? The reason you will frequently see cited is that most breast cancers occur in the upper outer quadrant of the breast. Because that quadrant of the breast is closest to the underarm, which is where antiperspirants are used, it must be the antiperspirants! And global warming is most definitely due to the decreasing number of pirates over the last three centuries. In fact, it is true that a little more than half of all breast cancers develop first in the upper outer quadrant of the breast, but it’s not because of antiperspirant use. It’s just because of a very simple fact of anatomy. Contrary to what people intuitively think when they hear the word “quadrant,” the distribution of breast tissue is not equal among the quadrants. In other words, each quadrant does not contain one-quarter of the breast tissue making up that breast. Rather, there is much more breast tissue in the upper outer quadrant than there is in other quadrants of the breast, because of a part of the breast known as the “axillary tail” or the “tail of Spence,” which consists of breast tissue extending toward the underarm. It turns out that the number of breast cancers diagnosed in the upper outer quadrant is proportional to the amount of breast tissue located there. There is no preponderance for upper outer quadrant cancers when the distribution of breast tissue in the different quadrants is taken into account.
The best evidence for a link is not so good
To me, the poor quality of evidence cited to support such a link between antiperspirants tends to be epitomized by an article that was being touted a few years back by Sharyl Attkisson. (You remember Sharyl Attkisson, don’t you?) At the time, she was touting an article by Dr. Kris McGrath in Medical Hypotheses, whose speculative nature and lack of peer review has been discussed elsewhere. I’ll start with this evidence and then work my way up to the best evidence cited by proponents of an antiperspirant-breast cancer link.
The evidence first cited is a study by McGrath in which he investigated a group of women with breast cancer and reported that the sooner they began using antiperspirants in their youth, the more frequently they used them, and the more frequently they shaved under their arms, the earlier they were diagnosed with breast cancer. Unfortunately this study was not very convincing. Besides being a retrospective study prone to recall bias, it had an enormous flaw in it, a flaw so obvious that I’m surprised this article got published. There was no control group. It’s a single-arm study that only looked at women who got breast cancer, and it didn’t control for a variety of confounders. For instance, women who started using antiperspirants or shaving earlier probably went through puberty earlier and, as a consequence, had their first menstrual period earlier. Starting menses early is a risk factor for breast cancer that has been known for a very long time. Ditto women who started shaving their underarms earlier. Worse, another, much better-designed study that did look at women both with and without cancer (and twice as many of each) had been published the year before and found no correlation between the use of antiperspirants and the risk of breast cancer.
According to McGrath, underarm antiperspirants clog the pores of apocrine sweat glands and cause the absorption of sex steroids into the blood. It’s a hypothesis that sounds very much like the one in the e-mail in which clogging the pores results in unnamed “toxins” backing up, just substituting sex steroids for “toxins.” It’s a pretty implausible hypothesis at best. The reason is that the amount of sex hormones made by the skin is dwarfed by what is made by the ovaries. Indeed, one of the main enzymes responsible for the production of estrogen in the peripheral tissues is aromatase. In the treatment of breast cancer, aromatase inhibitors don’t work in premenopausal women. The reason is that the ovaries of premonopausal women are still cranking out estrogens, which far outweigh the amount of estrogen produced in peripheral tissues. That’s why aromatase inhibitors are only used in postmenopausal women, where the ovaries have in essence shut down, leaving the aromatase in peripheral tissues as the only source of estrogen, which aromatase inhibitors shut down quite nicely. From a biological standpoint, it’s highly implausible that blocking the apocrine sweat glands can lead to a backup of sex hormones and their absorption into the breast tissue at concentrations sufficiently high compared to the normal levels made by the ovaries in women and the testicles in men.
Of course, “implausible” doesn’t mean “impossible,” and McGrath’s concept, although quite implausible biologically, is not as implausible as, say, homeopathy or reiki. However, because of its implausibility, it would take some pretty compelling evidence to make us as scientists reconsider our understanding of the biology. So does McGrath have compelling evidence or even highly suggestive evidence? Let this graph from his Medical Hypotheses paper speak for itself:
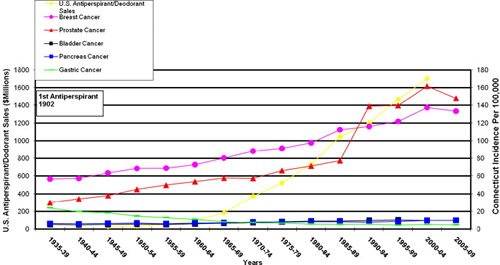
It’s very similar to this figure from the previous paper:

These are plots of antiperspirant sales in the U.S. versus the incidence of selected cancers, including prostate, breast, and a couple of others. Does this remind you of anything? Oh, this, maybe? It’s a beautiful example of the fallacy of confusing correlation with causation. It’s also amazingly sloppy in that the incidences of breast and prostate cancer were clearly increasing for at least two decades before the sales of antiperspirant started to take off, and antiperspirant sales have been increasing far faster than the cancer incidence rates shown. I also wonder if there was any attempt to control for common confounders, like age of menarche and number of live births per woman. Early age at menarche, increasing age of first childbirth, and decreasing numbers of children and up to nulliparity, all correlate with a higher risk of breast cancer. Regarding these factors, what have three major trends been over the last century? Earlier age of menarche, fewer children per woman, and an older age at first childbirth. Add to that the use of hormone replacement therapy during the 1980s and 1990s, and there are multiple huge confounders far more likely to explain the increasing incidence of breast cancer not even addressed in McGrath’s hypothesis.
OK, what else do we have?
Well, Joe Mercola referenced a couple of studies in his little bit of viral breast cancer fear mongering. Specifically, if you believe Mercola, it’s supposed to be the aluminum:
Research, including one study published this year in the Journal of Applied Toxicology, has shown that the aluminum is not only absorbed by your body, but is deposited in your breast tissue and even can be found in nipple aspirate fluid a fluid present in the breast duct tree that mirrors the microenvironment in your breast. Researchers determined that the mean level of aluminum in nipple aspirate fluid was significantly higher in breast cancer-affected women compared to healthy women, which may suggest a role for raised levels of aluminum as a biomarker for identification of women at higher risk of developing breast cancer.
The report discussed was a small pilot study of 35 patients, 16 with breast cancer and 19 with no cancer. While the results are somewhat provocative, it is important to remember that (1) the study was small and (2) the significance of the results remains unknown. More importantly, there were a lot of confounding factors not controlled for. For example, presumably for both women with breast cancer and those without in the study there was no serious attempt to control for confounding factors or to quantify the use of aluminum antiperspirants. Indeed, there are significant differences between the two groups. For example, the median age of the cancer group was 56, while it was 40 for the no cancer group. Perhaps something as simple as age could account for the difference. Does something happen after menopause leading to increased accumulation of aluminum from the natural exposure that we all have? Who knows? No analysis was done. Another possibility is that breast cancer might somehow accumulate aluminum more than normal tissue.
In other words, the study tells us absolutely nothing about whether or not aluminum-containing antiperspirants contribute to breast cancer risk.
Mercola’s next red herring is this:
In a 2007 study published in the Journal of Inorganic Biochemistry, researchers tested breast samples from 17 breast-cancer patients who had undergone mastectomies. The women who used antiperspirants had deposits of aluminum in their outer breast tissue. Concentrations of aluminum were higher in the tissue closest to the underarm than in the central breast.
Why is this a glaring red flag?
Aluminum is not normally found in the human body, so this study was a pretty clear sign that the metal was being absorbed from antiperspirant sprays and roll-ons. Please note that aluminum is typically only found in antiperspirants. If you are using a deodorant-only product it is unlikely to contain aluminum but might contain other chemicals that could be a concern.
Aluminum is not normally found in the human body? Did Mercola even read any of the articles he cited? The first article in and of itself demonstrated that aluminum is found in measurable quantities in normal human breast tissue nipple aspirates. Its finding was simply that it was found at higher levels in breasts with cancer. Then, the second article that there were detectable levels of aluminum in normal breast tissue, too! Again, what it purported to find was that there was more aluminum in areas of the breast closer to the underarm.
Here’s the study. Basically, in the study Exley et al. measured aluminum content in mastectomy specimens taken from 17 women with breast cancer. Four biopsies were taken, one from each quadrant, and measured the aluminum content. Suffice to say, there were huge variations between the concentration of aluminum in the fat and the breast tissue between individuals, so much so that, looking at the evidence, I can’t see a clear difference. The authors claim they found a “statistically higher concentration of aluminium in the outer as compared with the inner region of the breast” even though their statistics showed that there was not. Meanwhile, a followup study by the same group from 2013 found “no statistically significant regionally specific differences in the content of aluminium” and found that the concentrations of aluminum in patients with breast cancer were “comparable with those reported in non-diseased human tissues from other areas of the body.”
In a recent review article, Exley, try as he might, just can’t seem to develop a compelling case for the involvement of aluminum from antiperspirants (or anywhere else, for that matter) in increasing breast cancer risk. In another recent review article, Pineau et al. emphasize in vitro results but downplay the negative epidemiological and pathological evidence. Yes, aluminum might increase proliferation in MCF10A cells, which, contrary to what is claimed are not exactly “normal” (I’m well familiar with this cell line) and MCF-7 breast cancer cells, but there’s no compelling evidence that this has any relevance to the real world, given that there is no compelling evidence from epidemiology, pathology, and toxicology studies linking aluminum-containing antiperspirants with breast cancer. Moreover, there is good evidence that there is no correlation between the use of antiperspirants and breast cancer, and a comprehensive literature review failed to find convincing evidence of a link, concluding, “After analysis of the available literature on the subject, no scientific evidence to support the hypothesis was identified and no validated hypothesis appears likely to open the way to interesting avenues of research.”
In other words, although it’s possible that there is a link between antiperspirants and cancer, current existing evidence doesn’t support one and doesn’t even suggest potentially-fruitful avenues of research.
But what about parabens?
Of course, unlike the case among antivaccinationists, where aluminum fears supplanted mercury fears, in terms of breast cancer aluminum fear mongering is old school. New school is parabens. Parabens are hip. They’re now. They’re happening. In fairness, on the surface, there appears to be more of a reason to suspect them as potentially contributing to breast cancer than there is to suspect aluminum-containing antiperspirants. That’s not saying that there’s a compelling reason to suspect them, only that there is a modicum of plausibility. Parabens is a term used to describe a series of parahydroxybenzoates or esters of parahydroxybenzoic acid (also known as 4-hydroxybenzoic acid), chemicals most commonly used as preservatives by the cosmetic and pharmaceutical industries because of their bactericidal and fungicidal properties. They’re found in a variety of products including shampoos, commercial moisturizers, shaving gels, personal lubricants, topical/parenteral pharmaceuticals, spray tanning solution, makeup, and toothpaste. Most major brands of antiperspirant are paraben-free these days, but that doesn’t stop them from being examined as a cause of breast cancer. Typical of such articles is one by—you guessed it!—Joe Mercola entitled “Parabens: 99% of Breast Cancer Tissue Contained This Everyday Chemical (NOT Aluminum)“:
The featured study by Barr et.al. discovered one or more paraben esters in 99 percent of the 160 tissue samples collected from 40 mastectomiesiii. In 60 percent of the samples, all five paraben esters were present. There were no correlations between paraben concentrations and age, length of breast feeding, tumor location, or tumor estrogen receptor content. The median values in nanograms per tissue for the five chemicals were:
- n-propylparaben 16.8
- methylparaben 16.6
- n-butylparaben 5.8
- ethylparaben 3.4
- isobutylparaben 2.1
While antiperspirants are a common source of parabens, the authors note that the source of the parabens cannot be established, and that 7 of the 40 patients reportedly never used deodorants or antiperspirants in their lifetime. What this tells us is that parabens, regardless of the source, can bioaccumulate in breast tissue.
The study to which Mercola refers is this one by Philippa Darbre at the University of Reading. It’s one of multiple follow-up studies to a study by Darbre from 2004 that is thought to have started the concern about parabens. Basically, it measured the concentration of parabens in samples of 20 human breast tumors using high-pressure liquid chromatography followed by tandem mass spectrometry and found measurable parabens concentrations in all of them, with a mean of approximately 20 ng/g tissue. As noted by Joe Schwarcz, at the time the study received extensive press coverage, with few stories mentioning that there was no control group, making the significance of this observation unclear. That didn’t stop Darbre from promoting the idea that parabens cause breast cancer by pointing out that these chemicals have estrogen-like activity and that such activity has been linked to breast cancer. Since 2004, Darbre has built her career on doing studies trying to demonstrate that parabens and endocrine disrupters cause breast cancer, as a perusal of her PubMed publication list will easily demonstrate. She’s also co-authored articles examining aluminum-containing antiperspirants and breast cancer.
So, it would seem, we have a chemical that is widely used as well as a seemingly plausible mechanism (estrogenic activity) to cause breast cancer. There’s a problem, though. As Schwarcz, who is a chemist, also pointed out:
What she failed to mention was that the estrogenic activity of the various parabens is thousands of times less than that of estrogenic substances found in foods such as soybeans, flax, alfalfa and chickpeas, or indeed of the estrogen produced naturally in the body.
The study cited by Mercola was just the latest of her studies at the time. It suffers from the same sorts of problems as her 2004 study, although these problems are better hidden because more breast specimens were used and there was an attempt to correlate the parabens levels with location in the breast. One notes that, consistent with the 2004 study, Darbre found that every single breast specimen had detectable levels of parabens, even patients who didn’t use antiperspirants. I also note that “no direct, formal adjustment to the significance levels of the multiple Friedman ANOVA analyses has been made,” which makes me wonder about the actual statistical significance of the differences reported, particularly since the differences were so small and Darbre reports ANOVAs for each paraben, resulting in five different comparisons of four breast regions, one for each of the five parabens examined. For example:

Notice how small the differences are in general and how only one of the five parabens shows a statistically significant difference. The whole paper is like that, with multiple comparisons galore for the five parabens. Even though Darbre used an ANOVA, which is designed for multiple comparisons, for each paraben, she didn’t correct for the multiple ANOVA comparisons she did for each experiment. My guess is that, if she did, her statistically significant findings would disappear. Then there’s her observation that parabens levels did not correlate with tumor location, which rather argues against a correlation between parabens and breast cancer development. Most recently, Darbre has published an in vitro study of the effect of long term exposure (20 weeks) to parabens on the migration of breast cancer. It’s not clear to me how relevant these findings are to much of anything, given the lack of clinical evidence to demonstrate the relevance. None of this stops her from handwaving away all the problems with her studies and doing what, for example, antivaccinationists do when confronted with negative results: Invoke “individual susceptibility” without evidence for it.
Conclusion
Given how difficult it is in science ever to prove a negative beyond a doubt, it’s not impossible that something in antiperspirants, be it aluminum or parabens, might contribute to breast cancer development. However, given the existing state of the scientific evidence, it seems incredibly unlikely that there is a causal relationship here, given that no one has yet been able to convincingly demonstrate even a correlation. It’s certainly not for lack of trying. Indeed, scientists convinced of this hypothesis sometimes go to ridiculous extremes to show a “correlation,” as McGrath did in the graphs above.
Unfortunately, by far the most powerful predictors of breast cancer risk are not environmental. They are related to genetics (family history) and biology (age at menarche, age at menopause, number of live births, age at first live birth, breastfeeding, etc.). Lifestyle and environmental factors play a much less significant role, with protective effects due to exercise (for instance) or increased risk due to alcohol consumption (also for instance) producing much smaller effects than the previously mentioned risk factors and protective factors. None of this means that we shouldn’t study environmental risk factors for breast cancer, but it does mean that we should be cautious about spending too much time studying factors lacking strong biological plausibility when the studies aren’t yielding strong evidence of a correlation with breast cancer despite considerable effort to show a link.
It’s a matter of prioritization. Existing evidence is sufficient to conclude that there is no strong link between antiperspirant use and breast cancer and that there is very likely not even a weak link. Given such findings, it is appropriate to move on to other, more promising, avenues of research regarding environmental and lifestyle risk factors for breast cancer. This one’s been investigated and not found to be important.