{kind=link}
EDITOR’S NOTE: Dr. Arguello has responded. See his response and my reply here.
Not infrequently, I’m asked why it is that I do what I do. Why do I spend so many hours of my free time, both here and at my not-so-super-secret other blog (NSSSOB), to write my detailed analyses of various forms of quackery, analyses of scientific studies, and expressions of my dismay at the infiltration of pseudoscience into medicine, particularly medical academia in a phenomenon I like to call “quackademic medicine”? One reason, of course, is because I passionately believe in what I am doing. Another reason is that I want information countering various forms of dubious medicine to be out there, and I have two well-trafficked blogs as a platform, although SBM long ago surpassed my NSSSOB in traffic and reach.
Over the last six years, there are some topics that I’ve written about many times, such as the antivaccine movement, Stanislaw Burzynski, cancer quackery, and common myths about cancer treatment. Surprisingly, there are some topics left that I should have written about a long time ago but haven’t, even though I had heard of them before. One such topic, atavistic oncology and chemotherapy, was brought to my attention a couple of weeks ago by a reader, who basically pointed me to a particular dubious bit of cancer treatment whose chief proponent, Dr. Frank Arguello, is apparently currently touring Canada to do conferences and meet with potential patients, placing ads in local newspapers in the cities in which he will be appearing. His meeting with patients in Canada seems particularly problematic, because his cancer practice is located in San Jose del Cabo, Baja California Sur, Mexico, a location that, given the nature of his practice and claims, struck me as remarkable only because it’s not Tijuana. In any case, Dr. Arguello just appeared in Saskatoon on Friday and is scheduled to appear in Regina on July 30, with appearances in Winnipeg, Vancouver, Calgary, Edmonton, and Toronto promised in the future, as well as U.S. appearances in San Francisco and Los Angeles. Specifically, after his appearance in Regina, advertised here:
“Helpfully,” Dr. Arguello points out that he will be staying in Regina on July 31 to “meet with patients,” no doubt to try to recruit them to come to his clinic in Mexico to be treated. One wonders if he could be nailed for practicing medicine without a Canadian license. Be that as it may, what, exactly, is Dr. Arguello’s “atavistic oncology”? It’s a post I’ve been meaning to do for probably years now; so now is as good a time as any. It’s also because the hypothesis that cancer represents an “atavism,” the reawakening of ancient genetic programs seen in our single-celled ancestors billions of years ago, pops up periodically and sounds plausible. Unfortunately, virtually every example of this hypothesis is riddled with misunderstandings of evolutionary biology that render the hypothesis at best highly implausible.
Warning signs of quackery in Dr. Arguello’s atavistic oncology
It is important to differentiate two aspects of “atavistic” oncology. First, there is the hypothesis that cancer represents “atavism,” a reversion to an ancient evolutionary pathway seen in single cell organisms and early multicellular organisms. As I will discuss later, this hypothesis is not well-supported by the evidence and, in fact, represents active misunderstanding of evolutionary biology. The second issue is, assuming it is an accurate hypothesis, what atavism implies for the actual treatment of cancer. In other words, even if atavism is true, would Dr. Arguello’s proposed treatment actually target it in such a manner as to result in better outcomes than existing treatments? In that area, Dr. Arguello fails even more astoundingly, as you will see.
The first thing I noticed when I perused Dr. Arguello’s website is that it demonstrates a number of the warning flags of quackery. For example, one notes a paucity of clinical trial data published in the peer-reviewed medical literature supporting the efficacy of his methods, but one does see a lot of testimonials. If one looks at Dr. Arguello’s CV and his LinkedIn page, you find a seemingly-impressive list of positions before he became the director of the Dr. Frank Arguello Cancer Clinic, Institute of Science and Genomic Medicine, including:
- Assistant Professor of Pediatrics, Pediatric Hematology/Oncology Division University of Rochester School of Medicine and Dentistry (1990-1994)
- Senior Investigator, Laboratory of Drug Discovery, Research and Development Division of Cancer Treatment, Developmental Therapeutics Program, National Cancer Institute- FCRDC (1994-2000)
- Section Head of Preclinical Research & Development, Department of Drug Discovery Institute of Research Cesare Serono S.P.A ., The Ares-Serono Group (2000-2001)
An examination of Dr. Arguello’s CV and PubMed record rapidly reveals that his last peer-reviewed publication was in 2002, and that it was a review article. His scientific output, which had been pretty decent between 1988 and 2000. In academia, we sometimes see this sort of thing in doctors who decide to leave academia and go into private practice, but in the case of doctors like Dr. Arguello, who suddenly “discover” The One True Cause of Cancer and how to treat it, it’s a red flag suggesting unproven medicine at best and quackery at worst. In this case, it wasn’t until 2013 that he founded his clinic. In the meantime, he was busy starting a biotech business.
There’s even an offer to face a “public challenge” by conventional oncologists to demonstrate the efficacy of his methods by treating a patient with stage IV breast cancer, with the following criteria:
- The challenge will be advertised publically by the hosting institution (challenger), and communicated to the press, who shall monitor the results over time.
- The patient must have stage IV breast cancer. Other cases can be treated as long as a stage IV breast cancer patient is included in the challenge.
- The patient must have a Karnofsky Performance Scale above 80%, and documented evidence that she has not been exposed to conventional chemotherapy and/or radiotherapy.
- A neutral, non-biased review committee will review the protocol and publish the results.
- The challenging institution must cover all expenses for the patient(s), studies, medical honorariums, travel, etc., and must make all legal and regulatory arrangements for the study. Confidentiality agreements, disclaimers, etc., will be established.
- The challenging institution must have strong medical and scientific recognition to render a verdict that will affect the criteria of the medical and scientific community.
He even issued a press release for his challenge!
Of course, this is not the way things are done, and Dr. Arguello’s challenge is much like Jock Doubleday’s vaccine challenge in that it’s constructed in such a way that it’s unlikely that anyone will ever accept it, certainly not a reputable academic cancer center. This is not a clinical trial, much less a randomized clinical trial. No IRB worth its salt would ever approve such a “challenge,” because it is also totally unethical to offer an experimental therapy to a patient who hasn’t received standard-of-care treatment yet, given that there do currently exist effective treatments that at least palliate stage IV breast cancer. That’s particularly true given that Dr. Arguello doesn’t present any compelling preclinical evidence in cell culture or animal models to support his treatment. It’s even more of a problem, given that Dr. Arguello doesn’t even reveal the drugs and treatments he uses. Yes, you read that right. In a section of his patient brochure entitled “Drugs Employed & Their Use”, Dr. Arguello writes that he uses various FDA-approved drugs “off-label” to treat cancer:
The drugs used in combination have been selected based on the principles of “Atavistic Metamorphosis” published by Dr. Arguello in 2011, and after years of testing them in hopeless cancer patients. They fall in the pharmaceutical group of anti-bacterial (antibiotics), anti-fungal and anti-protozoal (anti-parasitic) drugs. Anti-viral drugs have also a place within the principles of Atavistic Chemotherapy because viruses preceded cells in their origin, and they were the precursors of the first cells on this planet. However, costs and toxicity of antiviral drugs have forced us to use them only when other approaches fail.
Because of delays in obtaining patents, the actual names of the medicines given in Atavistic Chemotherapy are not revealed to the patient. All of the drugs employed have expired patents since being in the market for decades. However, we are in the process of filing for patent protection for “New Use” or “New Formulation,” in order to protect the intellectual property and credit for this work. Although the drugs we use have been around for many years, Atavistic Chemotherapy and Immunotherapy is a new type of cancer treatment.
Another reason for not divulging the names of the medications is to prevent patients from self-medicating. It also prevents well-meaning caregivers from misusing drugs with which they are not familiar with in the treatment of cancer.
How humane. What rot! Sure, Dr. Arguello says that he’ll tell patients what the classes of drugs are that his patient receives and will offer them a hotline to find out exactly what the drugs are if they’re ever hospitalized and their doctors really need to know what they’re taking, but none of that helps scientists and oncologists to evaluate whether his treatments have any plausibility or likelihood of working. That’s the point. Of course, if any university were ever to accept a “challenge” from Dr. Arguello, he’d be forced to reveal exactly what his concoction is. Surely he knows this. In fact, in a way, Dr. Arguello is even worse than Stanislaw Burzynski. At least Burzynski apparently actually tried to do clinical trials before legitimate researchers decided they couldn’t work with him and he settled in 1997 on his model of using them to keep his clinic open and make money. Dr. Arguello doesn’t even seem to have done that.
But what is “atavastic oncology,” anyway?
Cancer as atavism: The resurrection of a very old idea
Perhaps the best way to explain what Dr. Arguello appears to mean when he describes “atavastic oncology” is to go to the source. Unfortunately (and not surprisingly), it’s a rather disjointed source, but it’s what Dr. Arguello claims; so we’re stuck with it. If you have time to go through it, there’s this 45 minute video:
On his website, there is this:
Cells in multicellular organisms have developed, over billions of years of evolution, complex and specialized cell functions according to their role in the body of multicellular organisms (skin cells, pancreatic cells, brain cells, etc.). We call these specialized cells “differentiated cells.” When differentiated cells lose their features of differentiation, they become “undifferentiated cells.”
We believe that when this happens, loss of differentiation features, cells reverse to their original, independent unicellular life form, and re-activate their basic functions of life: obtaining nourishment from the surrounding environment, reproducing themselves, migrating and spreading to ensure survival and perpetuation of life. This is what we call cancer. In other words, when a cell in a multicellular organism (animal or plant) reverts to its unicellular life form, cancer has developed. The resulting colony of reverted cancer cells will reproduce and spread inside the multicellular organism disrupting its functions and eventually causing its death.
And:
Atavistic metamorphosis proposes that cancer cells are cells that have reverted, evolutionarily, to their ancestral, independent status as unicellular organisms. It is from there that cancer only occurs in plants and animals/humans (multicellular organisms). This also explains why cancer does not occur nor can be induced experimentally in unicellular organisms such as bacteria, fungi and protozoa.
That last bit is about as silly as it gets. Of course, unicellular organisms can’t get cancer! Cancer, by its very definition as a set of diseases, requires a multicellular organism. Indeed, a seminal article from 2000 by Douglas Hanahan and Robert Weinberg described six hallmarks of cancer thusly:
- sustaining proliferative signaling
- evading growth suppressors
- resisting cell death
- enabling replicative immortality
- inducing angiogenesis
- activating invasion and metastasis
An update to this seminal work was published in 2011 and added additional hallmarks that had emerged over the last decade:
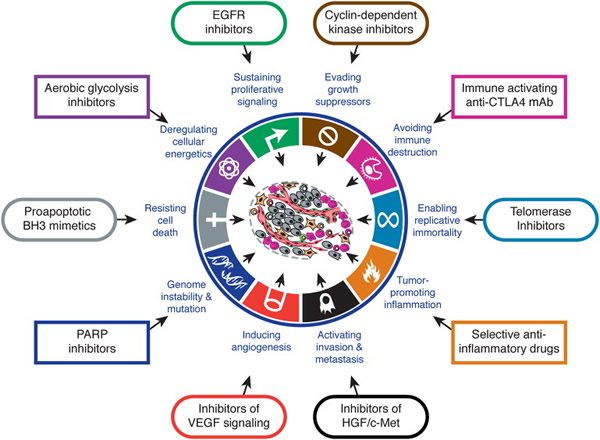
The point is that cancer is defined as a disease of multicellular organisms that results in a proliferating “organ” that doesn’t obey the rules that keep the rest of our cells growing when they’re supposed to grow, maintaining the structures they’re supposed to maintain, and staying in the parts of the body where they’re supposed to stay. Of course, unicellular organisms don’t get it!
It turns out that Dr. Arguello isn’t the only one promoting the atavistic hypothesis of cancer right now. In fact, two astrophysicists, Paul Davies and Charley Lineweaver, have been intermittently in the news for publishing a “unifying hypothesis” on the evolutionary origins of cancer. Back in 2011, for instance, Davies published an article in The Guardian entitled “Cancer: The beat of an ancient drum?” based on an article published by Davies and Lineweaver in Physical Biology entitled “Cancer tumors as Metazoa 1.0: tapping genes of ancient ancestors“. It turns out that the National Cancer Institute, in an effort to look at cancer in new ways, had recruited physical scientists to provide fresh insights. This was not a bad idea on its surface, but one consequence of bringing in people from unrelated disciplines is that they don’t know which hypotheses that have been considered before and rejected based on the evidence and therefore frequently act as though they were the first to have thought of a new hypothesis, as Davies does here:
With no prior knowledge of cancer, I started asking some very basic questions. What struck me from the outset is that something as pervasive and stubborn as cancer must be a deep part of the story of life itself. Sure enough, cancer is found in almost all multicellular organisms, suggesting its origins stretch back hundreds of millions of years.
Oncologists tend to think of cancer as a motley collection of cells gone berserk, but to me the way that tumours grow and spread to other organs indicates an organised and systematic strategy, designed to evade all that the body and the medical profession can throw at it. Such well-honed behaviour suggests they are the product of a long period of biological evolution.
I began wondering whether cancer might be an evolutionary throwback to the dawn of multicellular life, when single cells began cooperating and forming rudimentary aggregations.
And:
The reason that cancer deploys so many formidable survival traits in succession, is, we think, because the ancient genetic toolkit active in the earliest stages of embryogenesis gets switched back on, re-activating the Proterozoic developmental plan for building cell colonies. If you travelled in a time machine back one billion years, you would see many clumps of cells resembling modern cancer tumours.
The implications of our theory, if correct, are profound. Rather than cancers being rogue cells degenerating randomly into genetic chaos, they are better regarded as organised footsoldiers marching to the beat of an ancient drum, recapitulating a billion-year-old lifestyle. As cancer progresses in the body, so more and more of the ancestral core within the genetic toolkit is activated, replaying evolution’s story in reverse sequence. And each step confers a more malignant trait, making the oncologist’s job harder.
Note that this is merely a more “sophisticated”-sounding version of the same sorts of arguments that Dr. Arguello makes. Moreover, neither Lineweaver and Davies nor Arguello were the first to have thought of this idea. It’s a very old idea, indeed. Indeed, on Dr. Arguello’s site, there is a list of quotes from what he calls the “pioneers of atavistic metamorphosis,” including Rudolf Virchow, Herbert Snow, and Sir Henry Butlin, all of whom died at least over 84 years ago, with Virchow having made his name as the “father of modern pathology” back in the 19th century. In 2013, Darren Saunders pointed out that the idea that cancer represents some sort of devolutionary state dates at least as far back as Theodore Boveri, who 112 years ago published a fascinating article on the origin of cancer that, in part, discussed “interesting parallels” between malignant tumors and embryos produced by multiple divisions in the doubly fertilized sea urchin egg, as a suggestion of how tumors can resemble cells from early stages of embryogenesis. No wonder Saunders also likened the atavistic hypothesis of cancer from two astrophysicists to a doctor who reinvented calculus.
P.Z. Myers explained in depth why this line of reasoning was wrong, pointing out what any cancer biologist knows, namely that this “ancestral core of genes and processes deep in metazoan development” supposedly lurking, silenced, waiting to be switched on and to “turn the cell into a prehistoric monster” are not silent at all. They’re highly conserved (meaning that they’re so fundamental to cellular function that they developed very early in evolution and haven’t changed much) and active, controlling important developmental processes. They’re genes involved in cell division, adhesion, motility, and apoptosis (programmed cell death). As recognized by Hanahan and Weinberg’s hallmarks of cancer, they are the central controls that are disrupted in cancer and lose control over cell division. Moreover, Lineweaver and Davies, at least, totally misunderstand unicellular organisms when they argue that the ancient cellular program resurrected in cancer cells doesn’t “contain the genes that regulate cell proliferation.” Anyone who’s ever studied bacteriology would know that’s utter poppycock. Yes, even E. coli regulate their proliferation in response to a number of environmental factors, and there are bacteria that go completely dormant and form nonreplicating spores when environmental conditions are too harsh for replication.
The bottom line is that cancers are not most like single celled organisms. For one thing, they cannot survive outside of the body, leading Saunders to propose a test for the atavistic hypothesis: Drop tumor cells into the ocean and see if they live and grow, like ancient unicellular organisms could. In fact, most tumor cells can’t even survive for that long away from their fellow tumor cells in the body. The few that can are the ones that form metastases, but the vast majority of tumor cells that dislodge from the main tumor mass and get into the bloodstream die. Another limitation of the idea is the assumption that early metazoan organisms resemble tumor-like growths, which is simply not observed. As Saunders pointed out, cancers are dysfunctional by definition. I myself have written about how genetically messed up the genomes of cancer cells are on numerous occasions and how evolution drives the tumors to become more and more heterogeneous as they progress.
So what’s Arguello’s twist on atavism as the explanation for cancer? Well, I can’t read his book, although I could peruse a couple of chapters on Amazon. Well, his “reasoning, such as it is given that it’s based on an untenable hypothesis is this:
Atavistic oncology postulates that cancer cells are cells that have reactivated past evolutionary genetic information preserved in the genome (DNA). Thus cancer cells reacquire the abilities and behavior of their ancestral precursor cells, the primitive unicellular organisms. Therefore, malignant or pathogenic characteristics found in cancer cells such as unlimited replicative potential; capacity for invasion, migration, and metastases; abilities to evade the host’s immune system, and generate multidrug resistance; and abilities to live in hostile conditions are cellular traits reasserted from their hereditary past as primitive, independent single-celled organisms.
This does not imply that cancer cells are bacteria, or protozoa, or yeasts. It means that cancer cells express functions or behaviors similar to their ancestral parents, the unicellular organisms (such as bacteria-like and protist-like organisms) from which our cells originated.
If this is true, a combination of drugs that are effective to eradicate certain unicellular organisms should work in cancer treatment. Not only they should work, but this approach must be superior to any other approach used in the past to treat cancer. Because of the overwhelming results we have obtained and shown on our website, we prophesize that Atavistic Chemotherapy and Immunotherapy will become the way cancer is treated in the world.
So now we have the explanation for why Dr. Arguello uses anti-bacterial (antibiotics), anti-fungal, and anti-protozoal (anti-parasitic) drugs to treat cancer. It doesn’t explain why he uses antiviral drugs “when other approaches fail,” given that viruses are not considered to be unicellular organisms, given that they are not cells at all. Indeed, they are not even really considered to be alive, given that they cannot replicate by themselves and require a living host cell to do so. In fact, he even takes the idea that cancer cells are like metazoans and protozoans to the extreme that he thinks he can vaccinate against them by vaccinating against bacteria, while conceding, well:
Although unproven and totally speculative, we believe that the immune system can see and recognize molecular similarities on the surface among cancer cells, bacteria, protozoa and/or fungi. It is well known that vaccination for a given bacteria can indirectly protect the individual from other types of infections for different organisms not related to those in the vaccine. This is known as cross immune protection or resistance to phylogenetically unrelated organisms.
At least he admits this idea is totally unproven. But if that’s the case, then it’s even more unethical to use them as a basis of treatment without a lot more basic research and clinical trials. Would that he would admit the same for the rest of his ideas, but if you watched his video, you’d see that around 3:30 it’s claimed that Dr. Arguello can produce complete regressions of cancer.
Yes, cancer vaccines are a hot area of research right now. I happen to know researchers at my very own institution who are working on breast cancer vaccines, and I’ve served on the dissertation committee of a graduate student who was looking for ways to increase the efficacy of an experimental breast cancer vaccine. Vaccines are a promising area of research for some cancers. Here’s the problem. What Dr. Arguello is doing is not systematic or targeted, and my expressing my doubt is not, as he puts it, being skeptical about the idea that immunity against unicellular organisms or their toxins can crossreact against cancer cells and kill them. Rather, it’s against the idea that the reason this can happen is because tumor cells are atavistic, which is what Arguello argues. Indeed, it is striking how uncommon these observations appear to be (as demonstrated by the cherry picked papers included to bolster his point), other than the use of BCG as immunotherapy for bladder cancer, noted in a paper he misrepresents as having been published in Nature, when in fact it was published in a Nature journal, Mucosal Immunology.
What about the testimonials?
Leafing through the various testimonials included on Dr. Arguello’s website, I was struck at the resemblance of some of them to testimonials used by Dr. Burzynski. For instance, the case of Barb Juniper is an unfortunately typical case of a woman who developed melanoma, underwent successful surgical treatment, and then suffered a recurrence in the form of two brain metastases and a tiny deposit. These appear to have been surgically resected on January 24, although it’s not clear from the description (or the scans, for that matter), whether both or only one was resected. It’s also mentioned that an apparently-new frontal lobe metastasis was observed on March 4, but it’s also mentioned that an “abscess can’t be ruled out.”
The first thing I noticed is that many of these MRI slices are not at the same level and therefore not directly comparable. One of the lesions was clearly postsurgical change that resolved over the ensuing months. Another appeared to have shrunk in response to Avastin, although one can’t rule out atavistic chemotherapy having something to do with it. Of course, not knowing what drugs Dr. Arguello is giving, I don’t even know if his drugs cross the blood-brain barrier. I’m particularly shocked by this part of the testimonial:
He proposed to the patient a different approach in which for the first 30 days of the treatment the focus would be on reducing the blood flow and vascularity of the brain metastases to prevent bleeding during the actual atavistic chemotherapy and immunotherapy. This is called “Anti-Angiogenesis Treatment.” The patient accepted.
Dr. Arguello saw the patient on February 21, 2014, the same day she started the anti-angiogenesis treatment and continued until April 5, 2014 when the above treatment was discontinued and the atavistic chemotherapy and immunotherapy started.
One notes that we are not told which antiangiogenic therapy was used, but I can’t help but note that, paradoxically, bleeding is not an uncommon complication of certain antiangiogenic drugs. It’s all not particularly convincing.
Another case is that of a man with an indolent leiomyosarcoma of the leg that grew slowly over many years because he refused surgical intervention back in 2008 as the man sought “natural” (actually naturopathic) treatments. The series of photos (graphic!) to this surgeon show no obvious effect, and the patient abandoned treatment. There are several graphic series of photos of advanced breast cancer that might or might not have shown a treatment effect as opposed to the natural course of the tumor.
I like to think of it this way. If Dr. Arguello’s “atavistic” chemotherapy is as effective as he claims it is, it should be child’s play to demonstrate it in even a few relatively small clinical trials for different tumor types. He doesn’t. Instead, he cherry picks testimonials that might or might not show anything (it might be worth a separate post to analyze them individually) and issues nonsensical “challenges,” in essence, for others to do his own work for him. If he really did work as a pediatric oncologist at the University of Rochester and as a Senior Investigator in the Laboratory of Drug Discovery at the NCI, he knows these things. Yet he chooses not to do them. Instead, he does tours of Canada and the US looking for patients, doesn’t reveal what his protocols are, hiding behind a transparently deceptive excuse that he doesn’t want patients to “self-medicate” (and the more believable one that he doesn’t want other quacks to steal his ideas), and selling his cancer quackery at a clinic in Mexico.
There is a reason that atavistic oncology didn’t catch on among cancer researchers and physicians, and it’s not because of ideology and it’s not because of anyone “suppressing” the information. It’s because atavistic oncology is not consistent with well-established principles of biology and evolution based on 150 years of evidence. It’s because the hypothesis that cancer is an atavism provides no useful predictive power for treatment. Lineweaver and Davies might argue otherwise, claiming that atavism suggests treatments based on targeting the Warburg effect, DNA repair mechanisms, ABC transporters (which can function as drug efflux pumps), tumor-associated macrophages (TAMs), and immune interactions, a strategy they label as “target the weakness.” However, as a cancer researcher, I can tell you with knowledge that all of these “weaknesses” are already being investigated as potential therapeutic targets—and have been for at least the last decade—no appeal to atavism needed. Indeed, Lineweaver and Davies suggestion is downright insulting to cancer researchers who discovered the potential importance of these mechanisms in cancer and whose work Lineweaver and Davies seem to have inadvertently coopted as “just-so” stories that support their hypothesis.
Contrary to what Davies, Lineweaver, and Arguello seem to think, the reason the atavistic hypothesis of cancer hasn’t caught on is because it’s a hypothesis that is not new and has been considered and found wanting from a standpoint of biology and evolution. Unfortunately, it is a hypothesis that is easily co-opted for quackery, as Arguello has done.