{kind=link}
By Jean Brissonnet, translation by Harriet Hall
Note: This was originally published as “Placebo, es-tu là?” in Science et pseudo-sciences 294, p. 38-48. January 2011. It came to my attention in the course of an e-mail correspondence with the editors of that magazine, where one of my own articles was published in French translation in January 2015. I thought this was the best explanation of placebo that I had ever read. It covers the same points my colleagues and I have addressed and more. It describes the pertinent research and uses particularly effective graphs to illustrate the principles (a picture is worth a thousand words). The author, Jean Brissonnet, kindly gave his permission for me to translate it and share it with our readers.
In fact, you don’t need to give a placebo to get a placebo effect and therefore we can now think about how we can maximize the placebo component of routine care.
~ Damien Finniss, 2010
The scene takes place in a surgical suite where they are preparing to do a cataract operation. The patient is lying on the operating table. A few minutes earlier the anesthetic gel was applied to the cornea to permit an operation under simple local anesthesia. The surgeon arrives in the company of the anesthetist. They are engaged in a spirited discussion and don’t seem to be agreeing.
“It has been proven,” says the surgeon, “that 30% of the action of a medical treatment is due to the placebo effect.”
“I doubt that,” retorts his interlocutor, “I think that placebo story is one of those medical myths on a par with the idea that we only use 10% of our brain, that nails and hair grow after death, or that cellphones create interference in hospitals.”[1]
“No,” insists the surgeon with a superior tone, “the fact is established and has been proven by numerous studies.”
The anesthetist shakes his head with a slight smile, but he doesn’t reply. As for the patient, who might have much to say on the subject, he keeps quiet, because it would not be prudent to argue with someone who is about to suck the lens out of your eye.
This true anecdote would not be of interest if it didn’t concern two members of the medical profession. Why such uncertainty? Why such lack of knowledge about such a fundamental subject? This faith in an all-powerful, magical, and mysterious placebo is common among the general public and it serves as justification for resorting to unconventional medicines that have never been able to show solid proof of efficacy; but we see that it still persists among the medical profession.
To know whether the placebo effect is real or should be relegated to the same category as poltergeists, it will help to go back in history.
The history of the placebo effect
Although the placebo effect had long been recognized, official attention to it really followed the generalization of controlled clinical trials by the Cornell Conferences on Therapy in 1946. The popularization of this effect wouldn’t really occur until the publications by Beecher in 1955 and Haas in 1959.
Beecher reviewed 15 articles describing the treatment of 1,052 patients and estimated that across all the conditions studied, the average placebo effect was 32%. These results were confirmed by Haas a few years later based on 1,400 cases from 96 articles. He also found an average of around 30%, but he found a lot of variation depending on what was being studied. The improvement in the symptom of pain varied from 15% to 60%.
The consequence of these articles was the introduction of a simple additive model that considered the placebo effect as the difference between the global effect observed and the pharmacological effect. It was then defined as “the clinical effect produced by the administration of a placebo.”
This definition is important, because it attributes causality (“produced by”) to something that was really no more than a correlation. We had to wait a long time for that conception to be called into question. The reason for that was that the placebo effect was a little-known mechanism, because it had been little studied.
This lack of interest undoubtedly comes from the fact that the placebo effect competes with the actions of the doctor and takes away some of his credit for healing. In addition, the placebo is not interesting to the pharmaceutical industry that finances the majority of research. They are content to research the pharmaceutical effects of their products and don’t much care about other mechanisms of action.
Over half a century, there were around 20 studies on the placebo per se, and only a few hundred on the placebo in the context of pharmacologic studies. Consider this in comparison with the very many studies carried out on drugs.
The consequences of that state of affairs are numerous. They range from the highlighting, even in relatively recent articles, of old studies of questionable methodology, to the persistence of certain accepted ideas – including the famous 30% – and the unwillingness to question the models being used.
The authors of an article (Kienle and Keine,1997) that was one of the first to desanctify the placebo effect wrote, “False impressions of the placebo effect can be produced in various ways.” They cite numerous examples such as spontaneous improvement, fluctuation of symptoms, regression to the mean, additional treatment, scaling bias, answers of politeness, and many others. They find that “These factors are still frequent in modern literature on the placebo.”
Knowing that these authors analyzed over 800 articles, one can note that all references prior to this publication should be regarded with the greatest caution.
Questioning the placebo
This questioning comes from the fact that many researchers have not taken natural healing into account, which is curious considering how many pathological conditions heal spontaneously. For example, the journal Prescrire, in its February 2007 issue, wrote on this subject, “it can be estimated that without treatment, 50-70% of cases of simple acute cystitis resolve spontaneously, usually after having been asymptomatic for several months.”
In fact, what is called the placebo effect is the result obtained in a placebo control group (Figure 1).
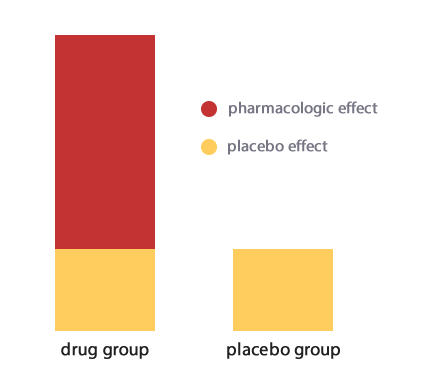
Figure 1
Therefore, it is necessary to conceptualize a new model in which the effect observed is equal to the specific effect of the medicine being studied plus a complex nonspecific effect in which the natural healing process plays a large part.
One will then have the scheme seen in Figure 2. The equation becomes:
Observed effect = specific effect + natural course of healing + a residual effect that we will provisionally call the placebo effect.
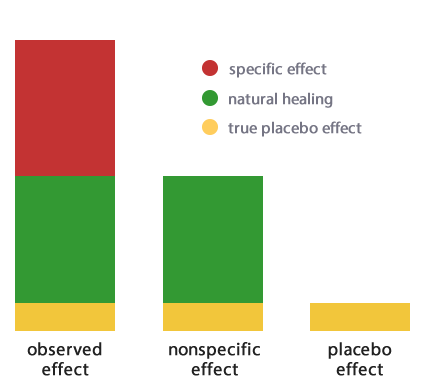
Figure 2
But isn’t this new “placebo effect” in turn composed of different elements? First among these are measurement errors made during the course of the trial. There are many such potential errors depending on the type of study. The best known are the phenomenon of regression to the mean, the Hawthorne effect, the Simpson paradox, the Will Rogers phenomenon, etc. (see box, below). Others come to mind: for example, an inaccuracy in the inclusion of subjects in the trial or the fact that patients tend to seek help when their symptoms are at their peak.
If all these measuring errors are subtracted, what remains can be called the “true placebo effect,” a term proposed by Ernst (1995), to distinguish it from the “false” placebo effect as traditionally conceived (figure 3).

Figure 3
The polemics
The resulting placebo effect is so reduced compared to the initial concept that some have gone so far as to question whether it exists at all. The first serious blow against the traditional understanding of the placebo effect was struck by Kienle and Kiene (1996).
The authors had the idea of repeating Beecher’s study to verify its validity. In their conclusion, they wrote:
Since 1955, when HK Beecher published his classic “The Powerful Placebo,” it generally has been accepted that 35% of patients with any of a wide variety of disorders can be treated with placebos alone. In recent years, average cure rates of 70%, and up to 100%, also have been quoted. It has been postulated that placebos can prolong life, that their effects occur in surgery as well as in medicine…In this article source material that forms the scientific basis for such claims is examined. Analysis shows that the studies on which such ideas are based, except perhaps in bronchial asthma, do not in any way justify the conclusions drawn from them. The truth is that the placebo effect is counterfeited by a variety of factors including the natural history of the disease, regression to the mean, concomitant treatments, obliging reports, experimental subordination, severe methodological defects in the studies, misquotations, etc; even, on occasion, by the fact that the supposed placebo is actually not a placebo, but has to be acknowledged as having a specific action on the condition for which it is being given.
Errors and Bias in Measurement
The Hawthorne effect: subjects may change their usual behavior just because they are participating in a study, and this can lead to overestimating the effects of treatment, particularly in the control group.
Regression to the mean: Including patients with very high or very low values at the beginning of a study gives the illusion that the statistical variation of subsequent measurements is improvement caused by the treatment.
Simpson’s paradox: When unrecognized determining factors (“confounders”) influence the data, the overall results of a study can be completely changed by analysis of sub-groups. [Translator’s note: another way of saying this is that a trend that appears in different groups of data can disappear or reverse when the groups are combined.]
The Will Rogers phenomenon: Improved diagnostic methods that artificially increase the prevalence of a disease can improve the apparent prognosis of a patient without the measurement parameters having been changed. [Translator’s note: If cancers are diagnosed earlier but there is no change the time of death, the survival time will appear to have increased. The name comes from a Will Rogers quotation: “When the Okies left Oklahoma and moved to California, they raised the average intelligence level in both states.“]
Taken from Kleist, P. (2006). “Quatre effets, phénomènes et paradoxes de la médecine. Leur signification et leurs racines historiques [PDF]. Forum Med Suisse; 6 :1023–1027.
And the authors are the first to say that “another error of judgment is the lack of clarity of the concept of placebo itself.” They conclude bluntly “that the literature relative to the magnitude and frequency of the placebo effect is unfounded and grossly overestimated, if not entirely false.” Finally, they raise the question of whether the very existence of the so-called placebo effect “is not in fact largely or totally illusory.”
This was like throwing a stone into a pond.
Nevertheless, neither this study nor the following article published a year later by the same authors on the same subject (Kienle and Kiene,1997) provoked reactions, even though they had all the requisite qualities and were published in peer-reviewed journals.
And yet, it is not for nothing that today “Beecher’s error” is commonly talked about! It was necessary to wait six years for another study, arriving at the same conclusions, to awaken the medical community out of its torpor.
In 2001, Hróbjartsson and Gøtzsche published an article based on 214 studies with a total of 8,525 patients. Their conclusions were as follows: “We found little evidence in general that placebos had powerful clinical effects…they had possible small benefits in studies with continuous subjective outcomes and for the treatment of pain.” And they concluded that “outside the setting of clinical trials, there is no justification for the use of placebos.”
This study, which goes against conventional wisdom, would be widely disputed, but the ensuing controversies would be very fertile.
To better understand this paradox, another team, Vase et al. (2002) repeated Hróbjartsson’s study, separating it into two meta-analyses depending on whether the purpose of a study was to use placebo as a control for an active treatment or to investigate the mechanisms of placebo analgesia. They show that the two groups Hróbjartsson studied were in fact two placebo groups, because the patients in a no-treatment group know they are part of a clinical study and they are regularly evaluated by doctors. So therefore, the use or non-use of a placebo “object” changes nothing. That’s why the authors propose a new definition: “The placebo response is the reduction in a symptom as a result of factors related to a subject’s/patient’s perception of the therapeutic intervention.”
It is therefore found that the terminology surrounding the famous placebo is extremely ambiguous, because it appears that the placebo effect is no longer linked to the placebo object and that this new definition requires that we distinguish “the placebo effect” from “the effect measured in the placebo group” and from “the effect of a placebo.”
We can’t hope to get the public to understand (or even the medical profession, which necessarily lacks the time to delve into these syntactical-semantic subtleties) unless we resort to a clarification and stop using the same word in several unrelated senses.
An attempt at clarification
It seems natural, in the current state of things, to distinguish two situations. In the context of a controlled clinical study, what matters is to determine the specific effect of the treatment. Everything else, which can be called “non-specific effects,” consists of complex elements and is of no interest to the sponsor of the study who is seeking to evaluate the specific efficacy of a given molecule (figure 4).
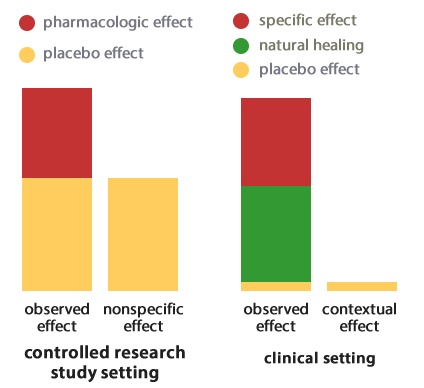
Figure 4
In the clinical context of treating a patient, on the other hand, the observed effect is equal to the pharmacological effect to which is added natural healing and an effect that we have called “true placebo,” but which, for the reasons indicated above, would now be preferable to call “contextual effect,”[2] as various researchers have proposed. (Di Blasi et al. 2003, Miller and Kaptchuk 2008).
Measurement errors have obviously disappeared from this context, which explains that the overall effect can be slightly inferior to that observed in the case of a clinical study.
Implementation of the contextual effect
It remains to understand what are the elements that can enter into play in the implementation and optimization of this contextual effect.
The first element is the therapeutic ritual: the results are different according to the route of administration, the taste, the name, the price, the color, etc. Several studies have confirmed the action of some of these parameters.
The second has to do with environmental conditions: the personality and beliefs of the patient, the attitude of his companions, the place where care is being administered, the attitudes of the treatment team, etc.
Finally, it seems that the most important element is the doctor/patient relationship.
In order to determine the influence of these three factors, to evaluate their relative importance and to see how they can be combined to provide clinical improvement, Kaptchuk (2008) studied three groups of patients suffering from irritable bowel syndrome. The first group was placed on a waiting list, the second received simple placebo acupuncture treatments, and the third received placebo acupuncture accompanied by special attention from the provider (a warm relationship, building trust, sustained attention). At the end of six weeks, they observed an improvement of 28%, 44%, and 62% respectively. The author concluded that “Non-specific effects can produce statistically and clinically significant outcomes and the patient-practitioner relationship is the most robust component.”
Psychological mechanisms
The psychological mechanisms involve two elements that can act simultaneously or separately: conditioning and suggestion.
Conditioning
Conditioning has been known since the work of Pavlov. He showed that if a dog becomes accustomed to the arrival of his food being accompanied by a sound stimulus, after a while the salivation reflex can be triggered by the sound alone in the absence of food. The same mechanism occurs when taking a placebo. As Gøtzsche (1994) wrote in The Lancet, “A lactose capsule has a greater effect in people who have previously reacted favorably to taking a benzodiazepine than in those who have never taken it.”
Suggestion
The power of suggestion has been known for a long time. One can cite its utilization by Mesmer under the fallacious pretext of an alleged animal magnetism or, closer to our day, by the famous Coué method.
More recent studies provide evidence of its role in the implementation of the contextual effect. Thomas (1997) followed 200 patients with functional illnesses. He divided them into four groups receiving either a placebo or nothing and either a positive or negative consultation. The first group received a placebo and a positive consultation (assurance of correct diagnosis, certainty of healing), the second, a placebo and a negative consultation (hesitation about the diagnosis, lack of confidence about the course of the disease), and the other two groups got a positive or negative consultation without a placebo. After two weeks, 64% of the patients who got a positive consultation had improved compared to 39% of those who got a negative consultation. But there was no significant difference between those who got or didn’t get a placebo. The improvement they found was therefore due to the suggestion created by the doctor and had nothing to do with taking or not taking a placebo object.
This clearly confirms that, as Bourreau and Coichard (2003) wrote, “It is useless to resort to a placebo to induce a placebo effect.” Which could be written more clearly today by saying that the placebo object is not necessary for the contextual effect.
Neurobiologic mechanisms
It is not enough to understand the psychological mechanisms that mediate between the context of care and the development of a therapeutic effect. We should also investigate how these psychological mechanisms are capable, in turn, of causing biochemical and neurobiological changes that can themselves produce measurable results.
Endogenous opioids
It is no coincidence that the vast majority of studies on placebo are performed in the area of pain, either artificially provoked or not. It is indeed in this area that one gets the most important nonsignificant effects. We can’t help but note the extreme importance of the contextual effect in relieving pain. This is why it was hypothesized that the observed effect was due to the secretion of opioids by the patient’s body. The results of studies on this subject are quite numerous and consistent. They confirm this hypothesis (see box, below).
The power of context in the treatment of pain
A study by Levine et al. (1981) perfectly illustrates the power of context in the treatment of pain. The authors studied the effect of intravenous morphine and intravenous placebo in 74 post-operative patients after extraction of impacted third molars. Two hours after the start of anesthesia, all patients openly received an intravenous saline placebo.* An hour later, each patient got either a second open placebo or a hidden dose of 4, 6, 8, or 12 mg of morphine administered automatically by a pump under double blind conditions. The level of pain was evaluated 50 minutes later using a visual analog scale. The average relief of pain after the second dose of placebo was found to be equivalent to that of a hidden dose of 4-6 mg of morphine and no patient got complete relief, even from that maximum dose of morphine (12 mg).
One can also cite, among the most significant studies, that of Petrovic et al. (2002), in which a light skin burn was induced in volunteers. They were divided into three groups who got either an opioid analgesic, a placebo, or nothing. In the patients who got relief from either the drug or the placebo, positron emission tomography (PET) showed an increase in activity in the rostral anterior cingulate cortex and in the brainstem, areas of the brain that are involved in the relief of pain. To confirm these findings, the patients were given naloxone (an opioid antagonist) and the pain returned.
*In an “open” intervention, the patient receives all the usual care from caregivers (putting medication in the intravenous line, verbal exchanges…). In a “hidden” intervention, the staff is not involved and the injection is given by an automatic pump, unbeknownst to the patient.
Neurotransmitters
Dopamine
It has been noticed that the contextual effect appears to be active in Parkinson’s disease. Parkinson’s disease is a condition that causes the degeneration of dopaminergic neurons, resulting in a deficit of dopamine in the nigrostriatal pathway that manifests clinically as a movement disorder.
De la Fuente-Fernandez et al. (2001) used labeled raclopride, a molecule binding to dopamine receptors, to detect dopamine receptors in the brain with PET scan (positron emission tomography). The patients received either an injection of levodopa[3] or placebo. They found that the placebo produced the same effect on dopamine receptors, triggering substantial release of endogenous dopamine in the brain. They concluded: “Our findings indicate that the placebo effect in Parkinson’s Disease is powerful and is mediated through activation of the damaged nigrostriatal dopamine system.”
It still remains to be seen whether these imaging findings translate into clinical results. A more recent study (Fregni et al., 2006) has modified the findings of the preceding study. It studied not just the patient’s subjective response, but also objective tests. The authors sought to investigate the immediate effects of two different kinds of placebo (a pill and sham transcranial magnetic stimulation) and compared them to the effects of standard treatment with levodopa. Subjective motor function was measured with a visual analog scale, and objective motor function was measured with a unified Parkinson’s disease rating scale (UPDRS). They concluded: “…placebo interventions in Parkinson’s Disease may have an immediate subjective sensation of improvement but result in no significant objective motor changes compared with levodopa treatment.”
Serotonin
Mayberg et al. (2002) carried out a randomized double blind study on 17 patients who were hospitalized for six weeks to test fluoxetine (an anti-depressant) against placebo. They did PET scans before treatment, a week later, and at the end of the sixth week. In each group, they found four patients who improved and who demonstrated increased activity in the part of the brain associated with emotions. However, the relief was less durable with the placebo.
Can placebos be used to treat patients?
We have just seen that the contextual effect is an essential element in terms of pain and probably also the various functional diseases. It affects subjective perception, but no evidence of action has ever been found in the areas of infectious diseases or tumors. As for the reality and the importance of its effects in Parkinson’s disease or depression, that remains unclear. It is obvious that the placebo, as an object, is useful in controlled clinical studies. In that setting, ethics committees require that the patient be informed and give informed consent. The problem that has been debated for a long time is the issue of its use in the clinic. There are many arguments against its use in healthcare practice. Do we have the right to fool the patient? Do we have the right to act without his consent? Can we risk permanently damaging the doctor/patient relationship if the patient finds out that he has been deceived? A better understanding of the phenomenon makes such questions obsolete. To the extent that the “placebo effect” is only a contextual effect that doesn’t depend on the use of an inactive object, it can and should be used in healthcare practice. It can probably be used instead of a prescription in certain functional diseases, and it certainly can potentiate the effect of prescribed drugs in many cases (analgesics, antidepressants…)
The authors of a recent study (Finiss et al., 2010) clarify this issue perfectly when they write, “For many years, placebos have been defined by their inert content and their use as controls in clinical trials and treatments in clinical practice. Recent research shows that placebo effects are genuine psychobiological events attributable to the overall therapeutic context, and that these effects can be robust in both laboratory and clinical settings. There is also evidence that placebo effects can exist in clinical practice, even if no placebo is given. Further promotion and integration of laboratory and clinical research will allow advances in the ethical use of placebo mechanisms that are inherent in routine clinical care, and encourage the use of treatments that stimulate placebo effects.”
So, then! Placebo, are you there? The placebo object is certainly there! It will be irreplaceable for the foreseeable future in carrying out the controlled clinical studies that are essential to medical research. As for the effect of the placebo, that doesn’t exist. As for the effect “called” placebo, if its existence is undeniable albeit limited, it would be better to simply name it “contextual effect” in order to better understand its true nature and to make its magical connotations disappear.
Notes
- These myths and many others are refuted in the article “Medical myths” BMJ 2007:335, 1288-1289 (22 December). return
- In the rest of this article, the term “placebo effect” will be designated “true placebo effect” or “contextual effect. return
- The international pharmacological name for L-DOPA, a substance used in the treatment of Parkinson’s disease that increases dopamine.return
References
- Beecher H.K., (1955) : The powerful placebo. JAMA 159 :1602-1606.
- Boureau F.and Cochard C.G. (2003) Douleur et effet placebo. La lettre de l’institut UPSA de la douleur ; 19.
- De la Fuente-Fernandez et at. (2001) Expectation and dopamine release: mechanism of the placebo effect in Parkinson’s disease. Science 293 :1164-6.
- Di Blazi Z. and Kleijnen J. (2003). Context effects. Powerful therapies or methodological bias ? Eval Health Prof 26:166-179.
- Ernst E., Resch KL.(1995). Concept of true and perceived placebo effects. BMJ 311: 551-553.
- Finniss G. (2010) Biological, clinical, and ethical advances of placebo effects. The Lancet 375: 9715, 686 – 695, 20.
- Fregni F. (2006) Immediate Placebo Effect in Parkinson’s Disease – Is the Subjective Relief Accompanied by Objective Improvement? European Neurology 56:4.
- Gotzsche PC. (1994) Is there logic in the placebo? Lancet 344:925-926.
- Haas (H.) et al. (1959) Das Placeboproblem. Fortschritt der Arzneimittelforschung 1: 279-454.
- Hrobjartsson A and Gotzsche PC. (2001) Is the placebo powerless? An analysis of clinical trials comparing placebo with no treatment. New Engl J Med 344:1594- 1602.
- Kaptchuk TJ et al. (2008) Components of placebo effect: randomized controlled trial in patients with irritable bowel syndrome. BMJ 336(7651):999-1003.
- Kienle GS and Kiene H. (1996) Placebo effect and placebo concept: a critical methodological and conceptual analysis of reports on the magnitude of the placebo effect. Altern Ther Health Med 2(6):39-54.
- Kienle GS and Kiene H. (1997) The powerful placebo effect: fact or fiction? J Clin Epidemiol 50:1311-1318.
- Levine JD et al. (1981) Analgesic responses to morphine and placebo in individuals with postoperative pain. Pain 10(3):379-89.
- Mayberg HS et al. (2002) The functional neuroanatomy of the placebo effect. American Journal of Psychiatry 159:728-737.
- Miller FG and Kaptchuk TJ. (2008) The power of context: reconceptualizing the placebo effect. J R Soc Med 101(5):222-225.
- Petrovic et al. (2002) Placebo and opioid analgesia– imaging a shared neuronal network. Science 295(5560):1737-40.
- Thomas KB (1987) General practice consultations : is there any point in being positive? BMJ 294:1200-1202
- Vase L et al. (2002) “A comparison of placebo effects in clinical analgesic trials versus studies of placebo analgesia.” Pain 99: 443-452.