{kind=link}
There used to be a time when I dreaded Autism Awareness Month, which begins tomorrow. The reason was simple. Several years ago to perhaps as recently as three years ago, I could always count on a flurry of stories about autism towards the end of March and the beginning of April about autism. That in and of itself isn’t bad. Sometimes the stories were actually informative and useful. However, in variably there would be a flurry of truly aggravating stories in which the reporter, either through laziness, lack of ideas, or the desire to add some spice and controversy to his story, would cover the “vaccine angle.” Invariably, the reporter would either fall for the “false balance” fallacy, in which advocates of antivaccine pseudoscience like Barbara Loe Fisher, Jenny McCarthy, J. B. Handley, Dr. Jay Gordon, and others would be interviewed in the same story as though they expressed a viewpoint that was equally valid as that of real scientists like Paul Offit, representatives of the CDC, and the like. Even if the view that there is no good evidence that vaccines are associated with an increased risk of autism were forcefully expressed, the impression left behind would be that there was actually a scientific debate when there is not. Sometimes, antivaccine-sympathetic reporters would simply write antivaccine stories.
I could also count on the antivaccine movement to go out of its way to try to implicate vaccines as a cause of the “autism” epidemic, taking advantage of the increased media interest that exists every year around this time. Examples abound, such as five years ago when Generation Rescue issued its misinformation-laden “Fourteen Studies” website, to be followed by a propaganda tour by Jenny McCarthy and her then-boyfriend Jim Carrey visiting various media outlets to promote the antivaccine message.
Fortunately, over the last three or four years, the media have become noticeably—and appropriately—much more dismissive of antivaccine pseudoscience. This seems to have occurred in the wake of Andrew Wakefield’s humiliation at being struck off (i.e., had his medical license revoked) in the U.K. and then having his infamous 1998 case series that started the fear mongering over a nonexistent link between the MMR vaccine and autism retracted by The Lancet based on evidence that he committed scientific fraud.
The antivaccine movement aside, there remains a temptation among scientists and government agencies to release the results of new studies having anything to do with autism either during the last week of March or the first week of April, all, of course, to take advantage of the publicity of Autism Awareness Month. So it was last week, when beginning on Thursday I sensed a disturbance in the antivaccine crankosphere force, with the antivaccine blog Age of Autism rerunning various posts by Mark “Not A Doctor, Not A Scientist” Blaxill and other AoA denizens from 2009. The reasons were obvious. The CDC was going to release the latest autism prevalence data on Thursday. The antivaccine crankosphere has been busily spinning those numbers since Thursday, which means it’s time to address those numbers here.
Autism prevalence in the United States, 2014
The CDC’s latest autism prevalence numbers was published in the Centers for Disease Control and Prevention Morbidity and Mortality Weekly Report (MMWR) in a report entitled Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years — Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2010. This is the sixth survey reported from data gathered from the Autism and Developmental Disabilities Monitoring (ADDM) Network. The ADDM is an active surveillance system in the US designed to provide estimates of the prevalence of autism and autism spectrum disorders (ASDs), as well as other characteristics, of children aged eight years whose parents live in eleven ADDM sites.
The goals of the ADDM are:
- To obtain as complete a count as possible of the number of children with ASD in multiple surveillance areas.
- To report comparable population-based ASD prevalence estimates from different sites every 2 years and to evaluate how these estimates are changing over time. To study whether autism is more common among some groups of children than among others.
- To provide descriptive data on the population of children with ASD.
The concept is simple; unfortunately the implementation is not. The report describes how surveillance is conducted at ADDM sites:
ADDM surveillance is conducted in two phases. The first phase consists of screening and abstracting comprehensive evaluations performed by professional providers in the community. Multiple data sources for these evaluations include general pediatric health clinics and specialized programs for children with developmental disabilities. In addition, most ADDM Network sites also review and abstract records of children receiving special education services in public schools. The second phase involves review of all abstracted evaluations by trained clinicians to determine ASD surveillance case status. A child meets the surveillance case definition for ASD if a comprehensive evaluation of that child completed by a qualified professional describes behaviors consistent with the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) diagnostic criteria for any of the following conditions: autistic disorder, pervasive developmental disorder–not otherwise specified (including atypical autism), or Asperger disorder. This report provides updated prevalence estimates for ASD from the 2010 surveillance year. In addition to prevalence estimates, characteristics of the population of children with ASD are described.
Why did the investigators choose age 8 as the benchmark, the age at which they would examine prevalence? As is explained later in the report, it’s because the baseline ASD prevalence study conducted by the CDC’s Metropolitan Atlanta Developmental Disabilities Surveillance Program (MADDSP) in 2003 demonstrated that this is the age of peak prevalence. How can that be? The authors of that study speculated that it was possible at the time that the lower rates in 9- and 10-year olds might have reflected the use of narrower diagnostic criteria for autism before the DSM-IV and the increased availability of educational and health services for children with autism in the 1990s. More specifically, prevalence rates in that study between the ages of 5 and 8 didn’t significantly vary from each other; so the investigators chose the oldest age in that range, in order to capture the highest prevalence rate. To that, I also wonder whether, as I pointed out multiple times before, the observation that some children lose their ASD diagnosis as they grow and develop had anything to do with it. Be that as it may, this is the system, and that’s how the estimates come about.
Last time the CDC reported these numbers, which was in 2012, they found that autism prevalence was 1 in 88. The antivaccine movement went wild. This time, in 2014, the CDC estimates that 14.7 per 1,000 eight year olds (1 in 68) have a diagnosis of an ASD. As Autism-News-Beat points out, this new estimate is 30% higher than the estimate from 2012. (It should be noted that this prevalence number comes from 2010 data.) It’s hard not to mention at this point that it’s very hard to blame this increase on vaccines given the stability of vaccination rates overall in the US. Let’s just put it this way: The increase in prevalence numbers is not a compelling piece of evidence that vaccines are the cause of an “autism epidemic,” no matter how much antivaccinationists try to convince you otherwise.
So what could be going on?
Making sense of the numbers becomes easier if you start looking at more than just the overall number of 1 in 68, or even the estimate that 1 in 42 boys and one in 189 girls living in ADDM Network communities were identified as having ASD in 2010. After all, we’ve known for a long time that boys are considerably more likely to be diagnosed with an ASD than are girls, and these numbers confirm that. So let’s look at more of the details:
Non-Hispanic white children were approximately 30% more likely to be identified with ASD than non-Hispanic black children and were almost 50% more likely to be identified with ASD than Hispanic children. Among the seven sites with sufficient data on intellectual ability, 31% of children with ASD were classified as having IQ scores in the range of intellectual disability (IQ ≤70), 23% in the borderline range (IQ = 71–85), and 46% in the average or above average range of intellectual ability (IQ >85). The proportion of children classified in the range of intellectual disability differed by race/ethnicity. Approximately 48% of non-Hispanic black children with ASD were classified in the range of intellectual disability compared with 38% of Hispanic children and 25% of non-Hispanic white children. The median age of earliest known ASD diagnosis was 53 months and did not differ significantly by sex or race/ethnicity.
Next, if you look at Table 2 in the CDC report, you’ll find a huge variation in the prevalence reported, ranging from 5.7 per 1,000 in Alabama (1 in 175) to 21.9 per 1,000 in New Jersey (1 in 46). Here are the data summarized in a graph:
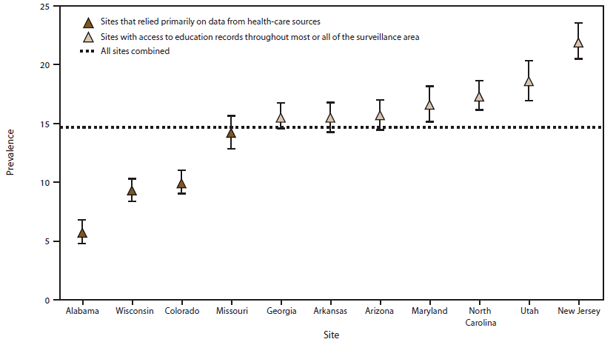
I noticed something about this graph immediately. Look at the colors of the data points. either dark or light. Notice the dark-colored points represent sites that relied primarily on data from healthcare sources, while the light-colored points represent sources that had access to educational records throughout all or most of their surveillance area? Why is that important? Simple: Notice how all the sites that only relied on data from healthcare sources (Alabama, Wisconsin, Colorado, and Missouri) report prevalence rates below the prevalence rate for all the sites combined. Only one (Missouri) had error bars that encompassed the overall prevalence rate for the entire ADDM Network. Now notice that the sites that had access to educational records (Georgia, Arkansas, Arizona, Maryland, North Carolina, Utah, and New Jersey) all reported prevalence rates that were either at or above the overall prevalence for the network. To me this is a red flag that at least some of the variability in the autism prevalence numbers has to do with the intensity of surveillance and the intensity of screening in various states. Frequently, this is mischaracterized dismissively by antivaccinationists as a huge straw man they like to call “increased awareness,” but in reality it’s a lot more than that, as I’ll discuss later. In the meantime, let’s move on.
Another red flag indicating that much of what is driving the changes in autism prevalence numbers is likely to be something other than biology is the wide disparity between autism prevalence as diagnosed in non-Hispanic Caucasians and in African-Americans as apposed to the much lower prevalence as diagnosed in Hispanics. Indeed, non-Hispanic white children were approximately 30% more likely to be identified with ASD than non-Hispanic black children and were almost 50% more likely to be identified with ASD than Hispanic children. This sort of disparity is far more likely to be due to differences in screening and diagnoses than to biology. Now couple this with observations in the report regarding ASD diagnoses as related to diagnoses of intellectual disability. The authors noted that in previous reports, from 2002 to 2008, the greatest increases in ASD prevalence were noted in Hispanic children, non-Hispanic black children, and children without co-occurring intellectual disability. The first two suggest that Hispanic and non-Hispanic black children are likely to be “catching up” with Caucasian children in terms of access to diagnostic services, while the increases in children without intellectual disability is interpreted thusly:
The much higher prevalence of ASD without co-occurring intellectual disability among white children appears to explain much of the variation in ASD prevalence estimates between different racial/ethnic groups. Among white children, the prevalence of ASD without intellectual disability was nearly double the prevalence among either black children or Hispanic children (OR = 1.8, p<0.01 for both comparisons). Conversely, the prevalence of ASD with co-occurring intellectual disability was similar among white children and Hispanic children but significantly higher among black children than among both of these groups. This suggests that in these seven sites, the significant white-to-black and white-to-Hispanic prevalence ratios were primarily driven by higher prevalence of ASD without intellectual disability among white children, and the significant black-to-Hispanic prevalence ratio was primarily driven by higher prevalence of ASD with co-occurring intellectual disability among black children.
In other words, more children without intellectual disability are being diagnosed with ASD. In the past, these children likely would not have been diagnosed with ASD—or with anything at all. Now they are being diagnosed. As Emily Willingham put it:
From the data, it looks like a lot of sociocultural factors enter into the values. Given the huge variability from site to site and the ethnic differences, recognition and service availability are probably factors. Dr. Boyle referred repeatedly to the evolution of our understanding of autism and used the large percentage of children included in these values who have average to above-average intelligence as an example of that. Unlike numbers from a decade ago, these values include children who previously might not have been recognized as autistic.
And Rachel Dornhelm:
For one thing, the prevalence seems to vary in different communities and among children of different races. The CDC found white children are far more likely to be identified with autism, even though scientists don’t believe the rates are truly different between whites, Hispanics or blacks.
That means that the discrepancy lies in the diagnosis and services available in different communities.
This is very likely true. As was pointed out in the analysis posted at the Thinking Person’s Guide to Autism, Richard Grinker studied ASD prevalence rates in South Korea and estimated that 1 in 38 children had ASDs there. In a news report about the study, Grinker pointed out that the reason the rates he found were so high was likely because in-person evaluations were performed for any child suspected of having an ASD and two-thirds of the cases of ASD identified in the study were “in mainstream schools, unrecognized, untreated.” If the estimates in the South Korean study are more accurate, prevalence rates for ASDs, which are clearly still underdiagnosed, can be expected to continue to increase for some time, until they finally level off at somewhere approximating the “true” prevalence rate. The study’s message, according to autism researcher Bennett Leventhal, is that “if you really go look carefully among all children everywhere, you find that things are far more common than you previously expected.” This is true not just of ASDs, but of pretty much every medical condition that has ever been screened for. If you don’t look for it, you won’t find it. If you do, you will, often at a much higher rate than you would ever have guessed.
I like to go back to an example I use time and time again. I use it time and time again because it’s about as good an example as I can find. Antivaccinationists like to use the argument that increased diagnosis and screening alone can’t explain such a large increase in a “genetic” disease. Thus, to them, autism can’t possibly be due to a genetic condition. Rather, it must be due to “environment”—cough, cough, vaccines, cough cough. However, as I believe to be worth repeating, they are quite wrong in the premise behind their argument.
If there’s a single rule I’ve learned over the last few years of looking into topics such as mammography, PSA screening for prostate cancer, or ultrasound screening for thyroid cancer, it’s that whenever a mass screening program for a medical condition—any medical condition—is undertaken, more people will acquire that diagnosis—sometimes many, many more. For example, let’s look at cancer, specifically breast cancer, since that’s what I know best in medicine.
I did a talk a while back in which I addressed this very issue; so I had to look up the data. Specifically, I looked at ductal carcinoma in situ (DCIS), which is a premalignant precursor of breast cancer. Basically, it’s cancerous cells that haven’t broken out of the breast ducts yet. What percentage of DCIS lesions progress to full-blown invasive cancer is not fully known, but it’s clear that some can and that some remain indolent, never endangering the life of the patient. Back in the early 1900s, DCIS was a rare diagnosis because by the time such lesions grew large enough to be a palpable mass, they almost always had become invasive cancers. (We can argue about whether only the lesions that progressed to cancer would grow large enough to produce a palpable mass or not; it’s quite possible that that’s largely the case.) Enter mammography. Now, thirty years or so after mass mammographic screening programs proliferated, DCIS is a very common diagnosis. Indeed, approximately 40% of breast cancer diagnoses are in fact DCIS. A recent study found that DCIS incidence rose from 1.87 per 100,000 in the mid-1970s to 32.5 in 2004. That’s a more than 16-fold increase over 30 years. Does anyone think that the “true” incidence of DCIS rose by 16-fold? Certainly I don’t. We have no evidence that would suggest that it increased by even two-fold. No, the increase in incidence of DCIS is nearly all due to intensive screening for cancer through the use of mammographic screening.
Think of something like hypercholesterolemia. Fifty years ago, it was an uncommon diagnosis. Changes in diagnostic criteria and screening have lead to an explosion in diagnoses, with large proportions of the population being on statins. Heck, before the 1920s doctors didn’t routinely measure systolic/diastolic blood pressure ratios; so there were few, if any, cases of hypertension because doctors weren’t looking for it. Even over the last decade, prevalence of hypertension has increased (for instance, in Canada). Perhaps a better marker for hypertension diagnoses is the percentage of adults who have been prescribed antihypertensive medications, which has skyrocketed since 1950. Of course, over that time, the definition of what constituted “hypertension” has changed markedly, to lower and lower diastolic and systolic pressures. Amusingly, various denialists lambaste such broadening of diagnostic criteria to claim that hypertension is an “engineered” epidemic, while denialists of another stripe (antivaccinationists) take advantage of the broadening of the diagnostic criteria for autism/ASDs in the 1990s to link the entirely predictable increase in ASD prevalence to their favorite bogeyman, vaccines.
Once again, definitions of medical conditions matter. They can have a huge influence on prevalence rates observed. Moreover, if you don’t look for something, you won’t find it, and if you do look for something, you will find a lot more of it than you expected. It is quite possible that that is what’s happening with autism, but such a narrative doesn’t fit into the vaccine-autism idea. The antivaccine movement needs an increasing apparent autism prevalence.
The antivaccine movement reacts
Predictably, based on the intense “preparation” by blogs like AoA, I wasn’t surprised to see that the antivaccine movement was ready to pull out the same sorts of histrionic reactions to this CDC report as it did to the CDC report two years ago. Predictably, SafeMinds denied that, well, I’ll let SafeMinds say it:
Katie Weisman of SafeMinds stated, “Broader criteria and awareness cannot account for this magnitude of increase. The federal government continues to spend millions of dollars ineffectively and ‘potentially duplicatively’ according to a recent GAO report. We need to identify environmental triggers for autism, prevent them, and develop effective treatments.”
Never forget that in anti-vaccine-speak, “environmental triggers” is a code word for vaccines. Weisman is also attacking a straw man, which is the straw man I alluded to earlier. The issue goes far beyond “broader criteria and awareness.” It involves both broader criteria and intensity of screening for developmental disorders, including ASDs. “Awareness” is too vague a term. Specifically, what likely accounts for the increased prevalence of ASDs includes a combination of broader diagnostic criteria, diagnostic substitution (i.e., conditions that formerly weren’t diagnosed as ASDs now fall under the the diagnosis of an ASD), and increased screening and concomitant availability of services.
If you don’t believe me when I say that “environmental triggers” is a code term for “vaccines,” just take a look at SafeMinds’ followup, Top Ten Things to Know about the CDC Report on Autism Prevalence. It’s a mix of self-reported weaknesses of the CDC report, such as the point that the ADDM sites were not selected to be representative of the US population and that ADDM sites change over time, making direct comparisons over time problematic. Of course, one can’t help but note that SafeMinds has no trouble assuming that the comparison between 2012 and 2014 (or 2010 and 2014) is perfectly valid, that autism prevalence really has increased 30% over two years, and that the difference couldn’t possibly be influenced by differences in ADDM sites. In any case, here come the antivaccine points:
Inaccurate Information Regarding Thimerosal Exposure: Thimerosal was not completely removed from vaccines in 2002. The concerns regarding the use of mercury (thimerosal) in infant vaccines surfaced in July of 1999 and it took several years for manufactures to alter their production process to remove or reduce thimerosal content. Vaccines that were being made during these transition years that contained thimerosal continued to be released with 2 year expiration dates, which means children in this report were still receiving thimerosal containing vaccines. Infants in high risk categories were also recommended to receive flu vaccines with mercury starting at 6 months of age and annually thereafter. In addition, the CDC Advisory Committee for Immunization Practices recommends that all pregnant women receive flu vaccines during pregnancy of which the vast majority contained mercury. The fetus accumulates mercury at higher levels than the mother and exposure to mercury during pregnancy is documented to cause neurological harm. Therefore it is impossible to report that there is no association between mercury in vaccines and autism prevalence.
The problem, of course, is that this study never said anything at all about thimerosal and autism. That’s not what it was designed to do. We have plenty of other studies that did look at that question to tell us that thimerosal in vaccines is not associated with autism. Nice straw man, though.
Of course, if it’s not thimerosal in vaccines, it must be the vaccines themselves, right? At least, so sayeth SafeMinds:
Given that the ADDM researchers had access to medical records, a valuable opportunity to evaluate immunizations, adverse reactions, and the development of autism has been ignored. We have had two decades of lost opportunities, which shows no sign of changing. The paper states,” Other topics of interest focus on socioeconomic indicators as well as perinatal risk factors such as timing of conception, weight gain during pregnancy, parental age, and interpregnancy interval.” The CDC failed to mention the many other factors which studies are showing increases autism risk, including air pollution, pesticides, proximity to toxic release sites, and medications such as acetaminophen and anti-depressants. While the CDC/HHS continue to tell the public that there is no link between vaccine injury (and exposure to mercury) and the onset of autism, a study conducted by EBCALA[3] and published in the peer-reviewed Pace Law Review confirmed that the government has compensated at least 83 families in the Vaccine Injury Compensation Program whose child suffered a vaccine induced brain injury resulting in the onset of autism.
In other words, SafeMinds is criticizing the CDC for not examining the hypothesis that they want the CDC to examine, a hypothesis that has been thoroughly discredited, citing a highly dubious “study” by a lawyer about legal claims whose conclusions were easily refuted and which was unethically carried out without institutional review board approval.
Meanwhile, AoA ramped up the nonsense with a series of truly silly Facebook memes. Perhaps the silliest of them all is this one:

To this, I reply, using my own specialty as an example: How could doctors in the 1970s have missed so many cases of DCIS? How could doctors in the 1950s have thought that the best treatment for breast cancer was a radical mastectomy? How could doctors in the 1960s not have realized how useful chemotherapy was for certain cancers? Medical science advances. The way I treat breast cancer now is actually significantly different than what I did 15 years ago, and how I treat it as my career is near to winding up in 15 years will likely be significantly different from how I do it now. The same is increasingly true of how it is diagnosed and characterized, given the rapid development of molecular medicine techniques being used to characterize tumors. Compared to 15 years ago when they did, today most women don’t have all the lymph nodes under their arms removed. Lots of them have chemotherapy first instead of after surgery. We do fewer mastectomies. There are new, targeted therapies. We can predict better who does and doesn’t need chemotherapy. For instance, as recently as ten years ago, a lot of women with node-negative estrogen receptor-positive cancers got chemotherapy based solely on the size of their tumors. Now, thanks to a 21-gene assay, we can much more accurately separate the women with such tumors not likely to benefit from chemotherapy from those who are and treat each accordingly.
My god, man! Those oncologists ten years ago must have been a bunch of idiots to have subjected so many women so unlikely to benefit to such toxic chemotherapy!
See what I’m getting at?
Of course, I love that scene from Star Trek IV: The Voyage Home, but, even as amusing as it is, it still annoys me to some extent, and that’s the assumption that doctors practicing in the past were somehow less intelligent, more ignorant, or even somehow “barbaric,” simply because they used techniques that we now know today to be inferior to what we have now. Doctors do the best they can with the medical and scientific knowledge of the times. The reason we still use chemotherapy, for instance, is because we haven’t (yet) found something that works better with lower toxicity.
The way we diagnose autism now and how we screen for it is different than it was 20 or 30 years ago, and arguably our understanding of it has greatly improved. That the autism prevalence rate from 10 or 20 years ago was much lower than it is now has nothing to do with pediatricians from 20 years ago being “a bunch of idiots” who “missed” so many autism diagnoses. It’s just that our understanding of autism and ASDs has evolved, as is the case with many medical conditions. Lots of what I learned in medical school 26 years ago is now obsolete. Lots of what I learned in residency 18 years ago is obsolete. Lots of what I learned in fellowship 15 years ago is now obsolete. Medical science advances and evolves, and physicians have to be continually learning to evolve with it. People who make arguments like this assume that all autism is the most serious kind, with obvious flapping, stimming, and other behaviors that define the most severe cases of the condition. Diagnostic criteria have broadened markedly since then.
Contrary to the hysteria over the numbers coming from the antivaccine crowd and, I should add, the rather clueless reporting that I’ve seen that stops at mentioning the 30% increase in ASD prevalence over two years and doesn’t delve into the nuances, these numbers do not represent a crisis. They do not represent evidence in support of a link between vaccines in autism. They don’t even really suggest a link between environment and autism. That’s not what this study was intended to do. What they do mean is that medicine is getting better at defining what autism is and diagnosing it and that there is still a ways to go, particularly in underserved communities and among underserved minorities. That’s why I agree with Shannon Des Roches Rosa. It’s time to keep calm and think critically, something antivaccinationists are unable or unwilling to do.
Now I just wonder if in 2016, I’ll have to do another post entitled Autism prevalence: Now estimated to be one in [insert next CDC report’s number here], and the antivaccine movement goes wild.