{kind=link}
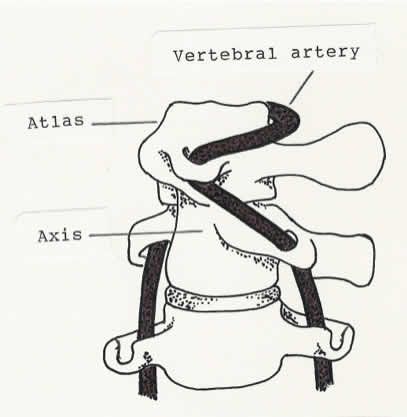
Extreme rotation of the atlas on the axis (at the atlantoaxial joint) stretches the vertebral artery. In layman’s terms, 40% of a hanging.
I am off to Chicago for 5 days to wow the SMACC crowd with my ID/SBM acumen. I hope. Given that most of my multiple-personalities do not seem to be able to get any work done, I am forced to write a brief post this week, limited by the battery life on my MacBook Air. Whatever I get down on paper? pixels? RAM? before the battery dies as I fly over the Rockies will be the post. It is times like this I wish I had Gorskian typing skills.
SBM has discussed the many limitations of chiropractic: the low grades for entry into chiropractic school, the inadequate training, their reason d’être, subluxations and their adjustments being divorced from reality, the lack of efficacy of chiropractic for any process beyond low back pain (and even that is no better than safer interventions), the fondness of chiropractors for other useless pseudo-medicines, and their opposition to vaccines.
Hm. When I put it like that chiropractic does appear a little sketchy. But is chiropractic safe? It is a hands-on intervention, for a brief period of time applying the same force to the neck as about 40% of hanging from the neck until dead. So there is certainly the potential for chiropractic to cause harm.
30-plus years in medicine have only reinforced the concept that under the right conditions, a perfect storm, even the most benign of interventions can kill. As an intern I had a patient whose IV, placed for an acute heart attack, became infected with S. aureus that went to her aortic valve that rapidly blew out and she died. There is always the potential of medical equivalent of Because a Little Bug Went Ka-Choo!
Can chiropractic care cause a stroke? No, because chiropractic care covers a lot of interventions, from the realigning nonexistent subluxations to the über-silliness of applied kinesiology and more.
Does neck manipulation, the high velocity, low frequency, amplitude (got the science-y terminology wrong the first time. Got to make sure the lipstick is correctly applied to the pig) neck snap of a brief hanging, lead to occasional stroke? Now that is the question.
Chiropractors love to point to the Cassidy study as the be-all and end-all evidence that neck manipulation does not cause stoke. It is the poster child for chiropractic motivated reasoning.
A careful reading, such I as did previously, suggests that the Cassidy study points to an increase risk for stroke following chiropractic, especially in the young. It was a flawed study, but if you are a chiropractor who doesn’t read carefully or beyond the abstract, you might think the paper supports the safety of chiropractic.
The authors of “Chiropractic care and the risk of vertebrobasilar stroke: results of a case–control study in U.S. commercial and Medicare Advantage populations” also admire the Cassidy study:
The work by Cassidy, et al. [32] has been qualitatively appraised as one of the most robustly designed investigations of the association between chiropractic manipulative treatment and VBA stroke
Which says something about the quality of the chiropractic literature and the safety of neck manipulation. But the study was done in Canada. What we really need is to reproduce the same lousy study in the US.
The paper looked at stoke 30 days following a PCP visit or a chiropractic visit for neck pain and found no difference in stroke:
Among the commercially insured, 1.6% of stroke cases had visited chiropractors within 30 days of being admitted to the hospital, as compared to 1.3% of controls visiting chiropractors within 30 days prior to their index date. Of the stroke cases, 18.9% had visited a PCP within 30 days prior to their index date, while only 6.8% of controls had visited a PCP
Which really says nothing. There is no information about why those who had a stroke were visiting either provider.
We do not know which patients had neck manipulation or even spinal manipulative therapy (SMT) since:
Less than 70% of stroke cases (commercial and MA) associated with chiropractic care included SMT.
Also:
There were statistically significant differences (p = <0.05) between groups for most comorbidities.
So it would appear that the two populations were not even remotely comparable.
Unlike Cassidy et al. and most other case–control studies our results showed there was no significant association between VBA stroke and chiropractic visits. This was the case for both the commercial and MA populations. In contrast to two earlier case–control studies, this lack of association was found to be irrespective of age. Although, our results (Table 8) did lend credence to previous reports that VBA stroke occurs more frequently in patients under the age of 45 years.
As the authors note:
Our results add weight to the view that chiropractic care is an unlikely cause of VBA strokes.
A conclusion based on comparing different populations whose intervention is uncertain. That is a “robustly designed investigation”? Perhaps chiropractic care is safe but how about neck manipulation? They are not the same thing. It is a fine point distinguishing between chiropractic care and neck manipulation, one that the authors recognize:
However, the current study does not exclude cervical manipulation as a possible cause or contributory factor in the occurrence of VBA stroke.
It is not death row care that matters, but that short drop through the trap door at the end. I suspect that the chiropractic organizations will fail to recognize this distinction.
I can’t see where the paper adds any information about the safety of chiropractic neck manipulation and will stick with the preponderance of data and the AHA/ASA Guideline.
But it does add FUD and I am sure there will be no end of blog entries trumpeting the paper and declaring that chiropractic is safe. It would appear that the approach to patient safety by chiropractors is embrace the good, yet flawed studies and rationalize away the bad, and who cares about patient safety when their subluxations need a fixin’.
The striking thing about chiropractic, and SCAM in general, is the aggressive denial that their interventions could and do cause harm, and the unwillingness to alter or abandon practices for increased patient safety.
Chiropractic advocates, and SCAM apologists in general, do love to mention the harm caused by NSAIDS or the deaths due to medications.
I have sat on hospital Quality Councils for 25 years as well as chaired my hospital’s infection control programs. I can proudly point to an enormous amount of work in that time to slowly drive down infections, morbidity and mortality. My hospitals are markedly safer than they were 25 years ago. This has occurred because we recognize that our interventions can harm and continually refine practice to minimize those risks. And because we apply the medical literature, always erring on the side of patient safety.
There still remains only one quality intervention to improve patient care in the entire SCAM universe, using sterile acupuncture needles, and the practice of acupuncture renders that intervention useless. Gloves are not high on their to-do list.
There are, to the best of my ability to locate, no other examples of SCAM practice being modified or abandoned due to evidence of harm.
And of course harm has to be balanced with efficacy. The first rule of medicine is not “do no harm.” Any and all interventions can harm. The first rule should be “on balance the good should outweigh the harm.” Chiropractic fails on that measure as well, since the benefit is negligible, applies only to low back pain, and is no better than safer interventions.
We do need better data. Many hospitals have stroke programs to maximize care for patients with stroke. When I last asked, the programs do not enquire into recent neck manipulation. Some clever epidemiologist needs to leverage information from all the stoke programs to help determine what the real risk of a brief hanging is.
And the pilot has let us know it is time to shut things down for landing. This is as good as it is going to get.