{kind=link}
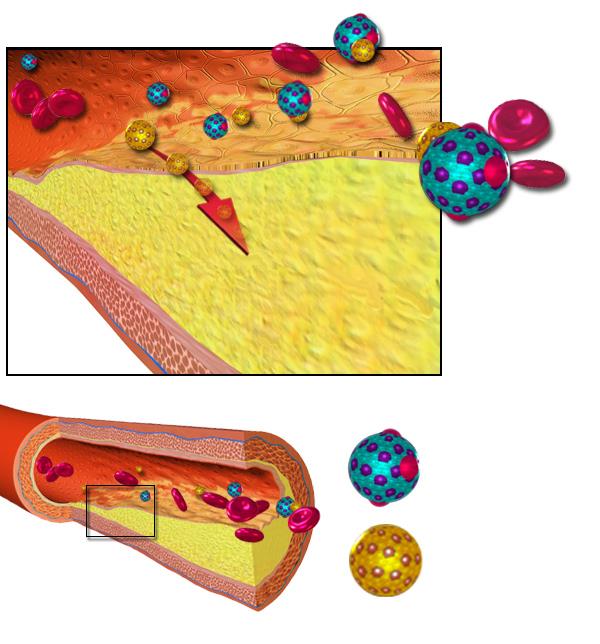
Pictured: The accepted theory of how high levels of cholesterol forms arterial plaques. Fat, in the form of low-density lipoproteins (yellow) deposits in the lining of the artery, eventually blocking it enough to cause symptoms.
![]() I’m really tired of arguing about cholesterol, but I feel obliged to stand up once more to defend science-based medicine from unfair calumny.
I’m really tired of arguing about cholesterol, but I feel obliged to stand up once more to defend science-based medicine from unfair calumny.
Lewis Jones’s article “Cholesterol-shmesterol” in Skeptical Briefs (December 2007) included errors and misconceptions about cholesterol. It was a re-hash of the same kind of misinformation that is being spread by The International Network of Cholesterol Skeptics (THINCS) and that I addressed in an earlier post. THINCS would like us to believe that cholesterol has nothing to do with heart disease; that low cholesterol is harmful and high cholesterol is beneficial; and they demonize statins, even falsely claiming that they cause cancer.
I answered Jones with my own article “Cholesterol Clarifications” in the June 2008 issue of Skeptical Briefs. I said I agreed that cholesterol does not “cause” heart disease, that low-fat and low-cholesterol diets have been promoted way beyond the evidence and that statins are being over-prescribed. The public has a lot of misconceptions, but thoughtful science-based doctors agree that the evidence shows:
• High blood levels of LDL cholesterol are a significant risk factor for cardiovascular disease.
• For primary prevention, lowering high LDL levels in high risk patients is associated with lower morbidity.
• For secondary prevention, lowering high LDL levels is associated with lower mortality.
• Low fat diet is only likely to lower LDL levels slightly (3-6% by one estimate).
• Statins are effective in lowering risk when prescribed selectively for patients at high risk, although the NNT (number needed to treat for one person to benefit) is relatively high.
Cholesterol Skeptic Marshall Deutsch didn’t like what I wrote. Skeptical Briefs published a dissenting letter to the editor from him. I will copy it in its entirety:
I don’t have at hand a copy of the article on cholesterol by Lewis Jones, but I recall that I found it interesting and accurate. Dr. Hall’s criticisms are conspicuously short of counter-factual evidence and long on irrelevancies (yes, physicians are dedicated to doing good, but that is not evidence for unwarranted concern over cholesterol.
This is not the first time Dr. Hall has demonstrated a dedication to defending what is clearly over-concern with cholesterol rather than considering the evidence for it. In a paper in Skeptic magazine in 2005 (Volume 11, No. 3), I presented data showing a clear and consistent inverse relationship between childhood mortality and blood cholesterol level. This is believable because cholesterol is an essential component of every cell membrane in the body, is a precursor of many essential hormones, and is a major component of brain tissue (about 25% of the cholesterol in the human body is in the brain). Dr. Hall dismissed the curve and data with the comment that I had combined data from developing and developed countries. This is true, but (1) within each group the data showed this relationship, and (2) I presented data from every country for which I could locate data, and I cited my sources. When this was pointed out, Dr. Hall presented no counter-evidence but noted that I am a member of an international group of investigators (Thincs) who had come together because we had each independently arrived at the conclusion that concern over dietary and blood levels of cholesterol is enormously greater than warranted. This seemed to imply that membership in such a group invalidates rather than reinforces our beliefs.
In the first place, Deutsch admits he doesn’t even have a copy of Jones’s article; he just “recalled” that he found it accurate. In the second place, I agree with him that the concern over cholesterol is far greater than warranted, and I said so quite clearly in my article.
It is disingenuous of him to say I was short on evidence. I summarized the current state of the evidence and mentioned the findings of several specific studies. I didn’t cite all the detailed references because the format of a Skeptical Briefs article directed to the general public was not the place to do that. I had already done that in a long Internet debate with Deutsch, which can be read in all its excruciating detail in the JREF forum archives. In that discussion, I pointed out defects in the studies he relied on and I cited original studies and meta-analyses to support my points. I directed him to the current science-based treatment recommendations in a review article in American Family Physician. I finally got him to agree with me on a series of points including that “the evidence for benefit [of cholesterol-lowering] outweighs the evidence against.” He said,
I agree with all your carefully worded points and with the abstract of the paper from American Family Physician, and would not be concerned about what seems to me to be pathological fear of cholesterol if it seemed that most physicians were as careful in their thinking as you and the AFP authors are.
After saying that, he acted as if he had never said any such thing and he went back to citing discredited studies. He even claimed that “Cholesterol is highly protective against cancer, infection and atherosclerosis” citing a study that didn’t even say that and that wasn’t even a study but simply an opinion piece.
What I said in the Skeptical Briefs article was equivalent to my “carefully worded points” that Deutsch had agreed with. He seems to have regretted his capitulation to evidence and logic. I don’t know what to make of that kind of backpedalling.
The Skeptic paper he refers to reveals his unique approach to science. He read that the NCEP (National Cholesterol Education Program) had issued a press release in 1991 recommending that the diet of children over 2 be modified to protect against cardiovascular disease later in life.
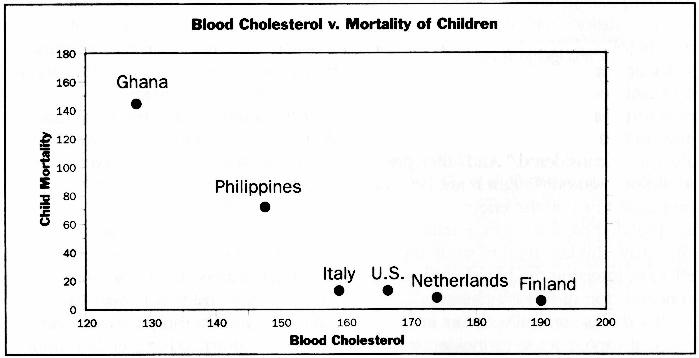
The press release was accompanied by a table showing a correlation between dietary cholesterol/saturated fat and blood cholesterol in boys age 7-9 in six countries. In Ghana and the Philippines, both dietary and blood cholesterol were low; in Italy, the US, Netherlands and Finland, both dietary and blood cholesterol were higher. The NCEP recommended that children over the age of 2 reduce their intake of cholesterol and fat in order to reduce the risk of atherosclerosis when they grew up. That may have been good advice for children at high risk but bad advice for the whole population. It may have inadvertently contributed to increased carbohydrate intake, poor nutrition, and obesity in American children.
These recommendations are open to valid criticisms; but instead of critiquing the recommendations rationally, Deutsch did some “research” of his own. He did it in the pages of the Encyclopedia Britannica. He looked up the death rates for children under the age of 5 in those 6 countries. He found that the lower the cholesterol in boys 7-9, the higher the death rate of children under 5. He concluded that it would be dangerous to lower dietary or blood cholesterol levels in children. By extension, and citing other cherry-picked data, he went on to claim that lowering high cholesterol levels in adults is a bad idea.
I think you will be interested to see what he calls a “curve” and “a clear and consistent inverse relationship between childhood mortality and blood cholesterol level.” It looks to me more like two isolated points and a small cluster.
Any statistician would be appalled at his methods and at this poor excuse for a “curve.” I don’t think I need to point out the flaws to readers of this blog. But for the purposes of discussion I’ll disregard all that. I’ll give him the benefit of the doubt and assume that the correlation between low cholesterol and high death rate in children is valid. What is clearly NOT valid is jumping to the conclusion he did. Has he forgotten that correlation doesn’t prove causation?
A more reasonable interpretation is that child mortality is higher in third world countries where there is more disease and malnutrition than in Europe. The association with low blood cholesterol levels is easily explained: we know those levels fall when people are malnourished or chronically ill. Cholesterol can be too low as well as too high.
No one has ever suggested that cholesterol is not essential to health. Our bodies can synthesize all they need as long as our diet is adequate. We need at least some fat in our diet. We need to maintain an adequate level of cholesterol in our blood. “Enough” is good. That doesn’t mean “too much” isn’t bad.
Anyway, all-cause mortality in children is not relevant to cardiovascular mortality in adults. Malnourished children with abnormally low cholesterol are more likely to die; but over-nourished adults with abnormally high cholesterol are more likely to die too. Deutsch’s own data on the four European countries tend to undermine his argument: Italy has the lowest cholesterol levels and Finland the highest; and we know adult cardiovascular mortality is much higher in Finland than in Italy.
I don’t think I’ve “demonstrated a dedication to defending what is clearly over-concern with cholesterol.” I think I’ve demonstrated a dedication to common sense and scientific evidence. I’d like to make it clear that I have no agenda here. All I’m interested in is what the evidence really shows. My cholesterol levels are OK, I don’t take statins, I don’t prescribe them (I’m retired), I have no ties to pharmaceutical companies, and I don’t worry about fat or cholesterol in my diet. I don’t have a dog in this fight. I would just like to know what the science really says.
I suspect that Deutsch does have an agenda: I suspect he is motivated to defend the reputation of The International Network of Cholesterol Skeptics, of which he is a founding member; and he has told me that his own cholesterol is very high and he has rejected the advice of doctors to lower it with statins. It’s only natural for him to want confirmation that he made the right decision. I have never said he should take statins. I have repeatedly said that a decision to take statins should be based on careful consideration of a patient’s entire risk profile and on a knowledge of the risk/benefit ratio for patients in that particular risk group. I recognize that taking statins is a bit of a gamble because of the high NNT. I recognize that different individuals given the same facts may legitimately choose different approaches. And I recognize that some individuals can tolerate a high cholesterol level with impunity because of their genes. Unfortunately we have no way of identifying those individuals yet. Deutsch may be one of those fortunate ones; I sincerely hope he is.
Finally, I wouldn’t characterize THINCS as a group of investigators; they do very little investigating and a great deal of propagandizing. I don’t reject Deutsch’s thinking because he’s a member of that group; I reject his and their thinking because it is flawed.
Yes, the general public is way too concerned about cholesterol and fat in the diet, too concerned about blood cholesterol levels and not concerned enough about other modifiable risk factors. But it’s clear that elevated LDL cholesterol levels are associated with increased risk of cardiovascular disease and treatments that lower elevated LDL levels reduce that risk. That’s what today’s evidence says. If tomorrow’s evidence leads elsewhere, I’ll gladly follow it.