{kind=link}
The evidence is clear: statin drugs are effective in reducing the rate of heart attacks and death in people who have already had a heart attack as well as in people who are at high risk of having one. Some people refuse to believe that evidence; they are statin deniers, similar to the climate change deniers and AIDS deniers (and there are even germ theory deniers!) who manage to disregard the strong evidence that proves their opinions wrong. The deniers demonize statins, cherry-picking studies to minimize the benefits and exaggerate the side effects.
A new study found that negative media reports about statins were correlated with patients discontinuing statin therapy. It also found that discontinuing statin therapy was correlated with an increase in heart attacks and death.
Statins work
I discussed the new guidelines for statin therapy in a previous post. I won’t repeat what I said there except to emphasize that the recommendations were made by a panel of experts who reviewed all the published evidence and arrived at a consensus. Panels of experts can be wrong, but if a denier is going to reject their consensus, he needs to come up with stronger evidence than the evidence the consensus was based on. The statin deniers don’t have that kind of evidence; they just re-hash studies that the experts knew about and took into consideration.
Criticisms of statins
There are some legitimate concerns. The effect size of statin therapy is not large; for every patient who benefits, a number of patients take them without benefiting (the number needed to treat or NNT varies with the individual’s overall risk status). Like any other effective drug, statins can cause side effects. And there are ways to reduce cardiovascular risk without drugs. (The guidelines emphasize other risk-reduction strategies, but if lifestyle changes don’t reduce the overall risk score enough, adding a prescription for statins is in order.) Some patients may rely on the protection of statins and be less motivated to lose weight, exercise, and stop smoking. Inappropriate prescription is a problem; some over-eager enthusiasts have even suggested statins should be added to the public water supply!
Then there are philosophical objections. There will always be room for informed patients to reject statin treatment for their own personal reasons. They may feel that the chance of benefit is too small to warrant the even smaller risk, they may not want to spend the money, they may know someone who had a serious adverse reaction to the drug, they may have ideological objections to solving problems with pills, they may have trouble swallowing pills, or they may have idiosyncratic reasons of their own that are hard for the rest of us to understand. Patient autonomy is the foundation of medical ethics; no one is going to force patients to take statins against their will. Science can’t tell people what they should do; it can only quantify the risks and benefits of doing it vs. not doing it.
The new study: methods
The new study was done in Denmark. That country’s Civil Registration System records births, emigration, immigration, and deaths for 100% of the population. Denmark also has a Registry of Medicinal Products Statistics that records data for all prescribed drugs, allowing the researchers to identify patients who were started on statins but did not continue getting them. The researchers examined the data on 100% of the individuals in Denmark who filled prescriptions for statins between 1995 and 2010. They excluded patients who started using them prior to 1995, those who started statins before the age of 40, those who took other cholesterol-lowering drugs, those who got more than 120 pills in the first dispense, and those who emigrated or died within 6 months of the first dispense. They were left with 583,349 patients who continued getting statins and 91,551 who didn’t. They did a nested 5:1 matched study to compare patients in the discontinuation group to patients in the continuation group, matching them for various characteristics in order to rule out possible confounders. They examined a number of factors that might have contributed to early statin discontinuation.
For the media analysis, they searched the Danish Infomedia database. It includes all news stories from Danish newspapers, magazines, radio, television, websites, and news bureau feeds, with dates of publication and textual transcriptions. The researchers found and read 1,931 transcripts and rated 110 as negative, 1,090 as neutral, and 731 as positive.
The effects of the media on statin use
They found a small but significant correlation between statin discontinuation and negative news stories. They calculated the odds ratio (with 95% confidence interval) for early statin discontinuation. After negative media stories appeared, the odds of discontinuation were 1.09 (1.06-1.12); for neutral stories 0.98 (0.96-1.01); for positive stories 0.92 (0.90-0.94).
Statin discontinuation increased risk of heart attack and death
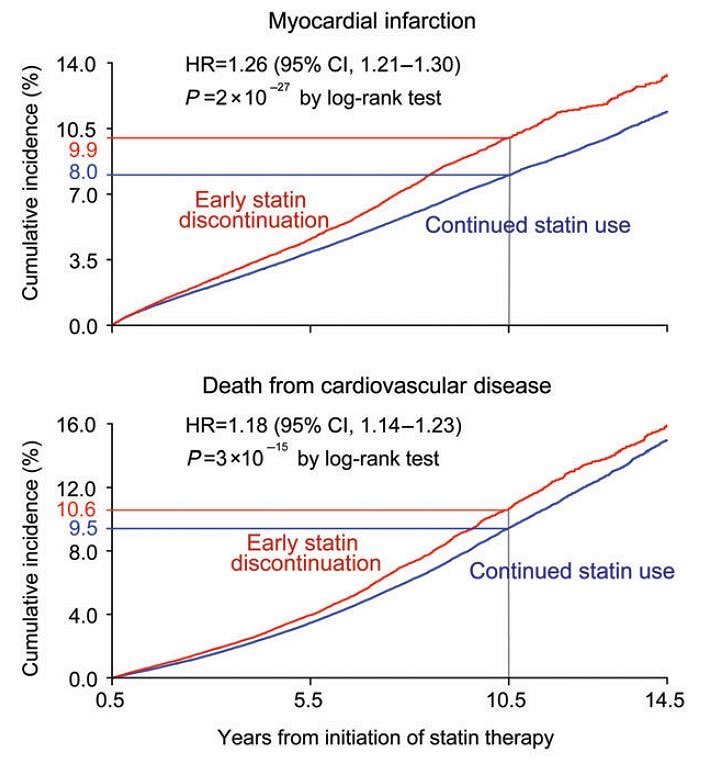
In the nested study comparing continuers to discontinuers, those who stopped taking statins were more likely to have a heart attack, with an odds ratio of 1.26 (1.21-1.30), and more likely to die, with an odds ratio of 1.18 (1.14-1.23).
Discussion: Limitations and denial
This study adds to the evidence that negative media stories can have an impact on medication use and on patient welfare. After the results of the Women’s Health Initiative study were publicized, the use of hormone replacement therapy (HRT) dropped and the rate of breast cancer dropped. After reports of a higher suicide risk in adolescents taking antidepressants, the prescription rate dropped and the rate of suicide increased, presumably because the drugs had actually been preventing suicides.
The correlation between negative media reports and statin discontinuation is small and is not that impressive. Correlation doesn’t mean causation; there is no way to know whether a patient had actually read the stories. We shouldn’t ever go by the results of a single study. The authors themselves pointed out the limitations of their study and warned that “great care should be taken in the interpretation of the present results.”
For me, the real importance of this study was the finding that patients who were prescribed statins had a greater risk of heart attack and death if they stopped taking them than if they continued. This should come as no surprise. We had good evidence that statins reduce the risk of heart attacks and death; it would have been surprising if the data had shown unchanged or reduced risk with discontinuation.
Statin deniers are already trying to discredit this study; among other things, they have accused the second author of bias because he declared that he received consultancy fees and honoraria from pharmaceutical companies. The study is far from definitive about the effects of the media, but it reinforces the already abundant evidence that statins are effective. The deniers don’t want to hear that message.