{kind=link}
 Case reports are perhaps the weakest form of medical evidence. They are essentially well-documented anecdotes. They do serve a useful purpose, however: they can illuminate possible correlations, the natural course of illness and treatment, and serve as cautionary tales regarding possible mistakes, risks and complications. I say “possible” because they are useful mainly for generating hypotheses and not testing or confirming hypotheses.
Case reports are perhaps the weakest form of medical evidence. They are essentially well-documented anecdotes. They do serve a useful purpose, however: they can illuminate possible correlations, the natural course of illness and treatment, and serve as cautionary tales regarding possible mistakes, risks and complications. I say “possible” because they are useful mainly for generating hypotheses and not testing or confirming hypotheses.
Dramatic case reports, however, with objective outcomes, like death, can be very useful by themselves in pointing out a potential risk that should be avoided. For example, case reports of objective and severe adverse outcomes are often used as sufficient evidence for pulling approved drugs off the market, or at least adding black box warnings.
The chiropractic community, it seems, does not respond in a similar way to dramatic adverse events that suggest possible risk from chiropractic manipulation. A recent and unfortunate case raises once again the specter of stroke following chiropractic neck manipulation. Jeremy Youngblood was 30 years old, completely healthy, and saw his chiropractic for some neck pain. According to news reports, Jeremy suffered a stroke in his chiropractor’s office while being treated with neck manipulation for the neck pain. According to reports the chiropractor did not call 911, but instead called Jeremy’s father who had to come and pick him up and then bring him to the ER. Jeremy suffered from a major stroke and later died.
According to his death certificate, which includes the findings of his autopsy:
I. Hemorrhagic infarction of cerebellum, mainly inferior surface, right, with obstructive hydrocephalus at the level of the 4th ventricle
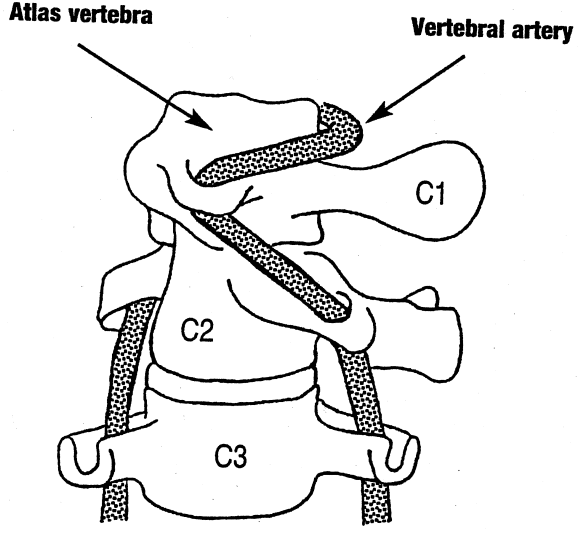
A. Status post right posterior/inferior cerbellar artery embolism with distal right vertebral right artery dissection at the skull base in C-1
B. Status post being coiled with a 6 mm x 20 mm Azure coil (x2), (status post coil embolisation of right vertebral artery)
C. Diffuse cerebral edema (weight 1600 gm)
D. Status post chiropractic manipulation of neck
A dissection is a tear in the artery. This tear can then result in the formation of a blood clot which can block flow through the artery or dislodge and plug a more distal artery, either way causing a stroke. In this case Jeremy had a stroke in the cerebellum, which is in the back of the brain just above the brainstem. The stroke also bled. This is a very dangerous situation, as swelling can damage the brainstem, and in Jeremy’s case also blocked the flow of cerebrospinal fluid out of the brain, leading to a further increase in pressure. This situation is often, and in this case was, fatal.
This is not an isolated case. There are other reports of patients having strokes right in their chiropractor’s office. There are now also several studies showing an association between chiropractic neck manipulation and vertebral dissection. The evidence is sufficiently concerning that the American Heart Association and the American Stroke Association recently came out with a statement which concluded:
Clinical reports suggest that mechanical forces play a role in a considerable number of CDs [cervical dissection], and population controlled studies have found an association of unclear etiology between CMT [cervical manipulative therapy] and VAD [vertebral artery dissection] stroke in young patients. Although the incidence of CD in CMT patients is probably low, and causality difficult to prove, practitioners should both strongly consider the possibility of CD and inform patients of the statistical association between CD and CMT, prior to performing manipulation of the cervical spine.
What they are saying is that there is sufficient evidence to be concerned that CMT can cause a dissection in a young patient resulting in a catastrophic stroke, even death. While the overall risk of this occurring is probably low, at the very least practitioners should obtain informed consent and disclose this risk before performing CMT. We have not had the kind of definitive controlled trials to prove that the neck manipulation is causing the dissection because it is possible that the neck pain itself was caused by the dissection which occurred before the CMT. It seems unlikely, however, that this explains every case, as with this one, in which the stroke occurs in the chiropractors office. Even if the dissection was pre-existing, that would be a contraindication to manipulation, which can turn a dissection into a stroke by making it worse or dislodging a clot.
I would go much farther than the AHA/ASA statement. In medicine we must consider the risk vs benefit of every decision and intervention. In this case there is no evidence the CMT is of any therapeutic value for neck pain, headache, or any indication. A systematic review of the evidence concludes:
Done alone, manipulation and/or mobilization were not beneficial; when compared to one another, neither was superior.
There are many gentler alternatives for neck pain, such as exercise, moist heat, or gentle massage. No matter how you look at it, there is no justification for chiropractic manipulation of the neck. Any risk is not justified when there is insufficient evidence to support efficacy and when there are safer options available. In this case the risk may be rare, but the adverse events are catastrophic — stroke or death in otherwise-young, healthy people.
If CMT were a drug, it would have been pulled off the market. If it were a common medical procedure, there would be more studies exploring the risk and more definitively answering the question of safety and efficacy. The response of the chiropractic community to the issue of neck manipulation and stroke, however, is denial and diversion. According to a KFOR article reporting Youngblood’s death:
Chris Waddell is the President of the Oklahoma Board of Chiropractic Examiners. He says their work speaks for itself.
“I think if the benefits weren’t there, people wouldn’t utilize our services. They know what works and what doesn’t,” Waddell said.
Wadell says data doesn’t back up the idea that visits to the chiropractor can kill.
The data he’s referring to is the Cassidy Study, which was done in Canada years ago.
“We found no evidence of excess risk of VBA stroke associated chiropractic care compared to primary care,” the report states. “For those 45 years of age and older there was no association.”
The notion that patients know what works is a common defense of alternative practitioners, or anyone using a treatment that is scientifically dubious. The claim is that patients would not seek out a treatment unless it actually works. This is demonstrably untrue, however. History is full of examples of worthless and even harmful interventions that were popular. Placebo effects are sufficient to explain the popularity of a worthless treatment.
Waddell also refers to the Cassidy study, which was a scientifically terrible study (as Mark Crislip explains here). This is a good example of cherry picking low grade evidence in favor of better or more comprehensive evidence. As the quote above indicates, the Cassidy study found no association with those 45 years and older. The study, however, looked at all strokes, not just those associated with arterial dissection. Also, by looking at the older population, any signal of association with chiropractic manipulation would be statistically drowned out by the far more common causes of stroke in the older population. The Cassidy study is essentially useless, but chiropractors love it because it gives them the cover they seek.
In another study, only vertebrobasilar strokes were examined, in those <45 years old. They found that patients with such strokes were 5 times more likely to have visited a chiropractor in the last week than a control population.
The Oklahoma Chiropractic Association also put out this statement:
The Oklahoma Chiropractors Association wishes to express its deepest condolences to the family of Jeremy Youngblood. The loss or harm of any patient is a very disturbing circumstance that medical professionals have struggled with throughout history. Unfortunately, there is no single form of medical care without risks.
Oklahoma Chiropractors are proud to provide thousands of Oklahoman’s drug free medical care daily. The safety of chiropractic care is evident by the lowest medical malpractice insurance rates of any licensed medical profession.
This is another piece of masterful denial and diversion. First they depersonalize this case – harm happens, no intervention is without risk. Then they tout the safety of chiropractic overall. Of course it is easy to claim safety when you ignore or deny risk. The issue here is relative risk vs benefit. There is a serious claim being made by healthcare professionals and organizations, based on existing evidence, that chiropractic neck manipulation carries risk that is not justified by the benefit.
Conclusion: there should be a moratorium on neck manipulation
The chiropractic profession has a responsibility to deal with this issue in a way that is best for their patients, not their profession. In my opinion the current evidence supports the following measures:
- Call an immediate moratorium on neck manipulation for any indication.
That’s it, actually. I don’t see how any other reaction would be appropriate. However, short of simply abandoning this procedure, other measures would at least be helpful:
- At least end the most forceful types of high cervical manipulation.
- Gentler forms of manipulation should be carefully studied for safety and efficacy with rigorously-designed trials capable of detecting adverse events.
- Require informed consent by patients prior to any neck manipulation. The consent should fully inform patients about the risks of dissection and stroke.
- Chiropractic organizations should publish standard of care guidelines that are strictly evidence-based and that err on the side of patient safety and minimizing harm.